Robert Prost emails:
I wanted to share with you, my take on the corona virus situation in the United States.
But first, a brief introduction. I am professor emeritus at the Medical College of Wisconsin in Milwaukee.
I have a PhD in Biophysics and spent my career in MRI-based research, mostly on brain tumors.
I check the Johns Hopkins’ website every day for the progress of the epidemic and I had a feeling about the numbers I’ve been seeing.
The website: https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 is very good.
The daily case number totals can be extracted by mousing over each plotted point in the graph in the lower right hand corner of the screen.
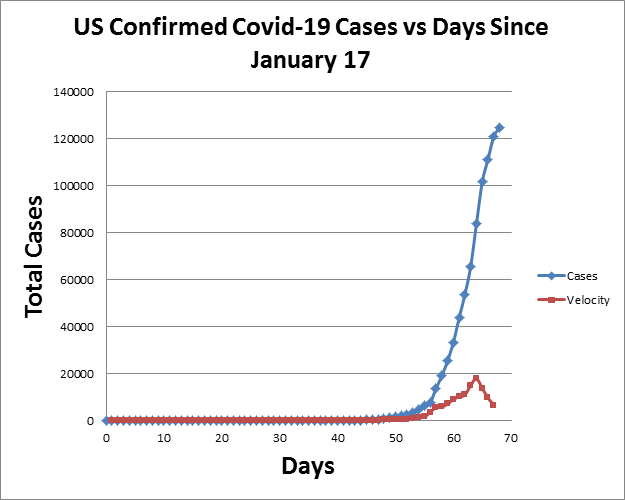
The curve at first looks daunting, it seems to be shooting straight up. But being at least in part a mathematician, I wondered about the velocity of this upward move in cases.
If the velocity was going up, the epidemic would be accelerating, the epidemic would be worsening. If going down, it would be getting better (slowing).
So I plotted the data and took the first derivative with respect to time. What it shows is that the velocity of the epidemic in the US is definitely slowing, and quickly.
While the number of confirmed cases continues to rise, it is rising more slowly. If there were a confounding effect from increased surveillance (more testing revealing yet more cases), the apparent velocity should be going up.
Instead, it is going down. So I believe the effect to be real, and thus I believe we are witnessing the beginning of the end of the epidemic. While this data says nothing about the potential for re-emergence in the fall or following spring, it does suggest that we have in fact, flattened the curve.
UPDATE: A follow-up email from Robert is posted here.
Interesting. But it is not clear that the number of “cases” is a useful metric — because the number of “cases” depends as much on the spread of testing as on the spread of the virus. And we also have to remember that the majority of people who test Positive for the virus (and thereby become a “case”) have no or only minor symptoms.
We also need to keep a sense of context and scale. 125,000 total Covid-19 cases sounds bad — until we recognize that so far this flu season, there have been 38,000,000 cases of the flu, resulting in 390,000 flu-related hospitalizations and 23,000 deaths. And this is considered to be a fairly light flu season!
The most useful metric would be a statistically significant increase in total “All Causes” daily or weekly deaths. For the countries for which that kind of data is available, there has been no such increase.
That looks like an improvement. The testing is especially slow in CA but that will only affect final CFR, not the rates.
Bad news, the University of Wisconsin at Milwaukee doesn’t have a medical school, that is in Madison. Funny, I would expect the professor would know that. Disinformation is another pandemic we need to be aware of.
“Disinformation is another pandemic we need to be aware of.”
Indeed:
https://www.researchgate.net/profile/Robert_Prost
https://www.researchgate.net/institution/Medical_College_of_Wisconsin
The key number we need, and don’t have, is just how prevalent the virus actually is in the general population, right now.
My guess is that if we hadn’t had all the publicity, the entire “pandemic” would have vanished into the background noise as part of the annual flu season, and we’d have written it off as a particularly bad one–Until someone went back and did the work to determine what made it so bad.
I think we really need to take up that idea that doctor in Seattle was working on–Survey the population and sequence what’s actually out there and making them sick. Not to mention, start testing the hell out of everyone coming into the country from the world’s disease reservoir.
Aside from the H1N1 epidemic, which I remember as being traced to Mexico or Central America, every single major influenza epidemic in the last hundred-plus years has come out of China or Southeast Asia. It’s past time for us to get a clue, and either begin cutting off access to that region, or taking steps to get accurate information out of there in order to make wise decisions about what we do.
Had we not “opened up China”, this would likely have been a blip on the radar, as it would not have spread outside the confines of the Bamboo Curtain with anywhere near the speed this has. Modern travel and communications absolutely must be curtailed to a point where we can cope with the attendant epidemic disease issues. This isn’t the “good old days” where you could force ships arriving to undergo quarantine before entry, and we’re going to have to find modern equivalents.
Funny Jonathan but in all the years I’ve read Chicago boys I thought you were a lawyer.
If the spread is indeed going down that is good news. I’ve heard with most pandemics there’s at least two or three waves over a year to two years-is that true?
I am conflicted over exactly what this is. We’ve had more deaths from common flu than this and yet it is touted as being so terrible. I think if the media hadn’t been trumpeting this on and on ad nausea we wouldn’t be shutting the country down.
@Kirk – “My guess is that if we hadn’t had all the publicity, the entire “pandemic” would have vanished into the background noise as part of the annual flu season, and we’d have written it off as a particularly bad one–Until someone went back and did the work to determine what made it so bad.” I have been pounding the table on this point from the very start and agree 100%.
Q anon. You’ve got your schools mixed up. The Medical College of Wisconsin is attached to a Froedert Hospital, our major Trauma center. Everyone living here in Milwaukee knows just how prestigious the Medical College is and that it is recognized nationally. YOU are the source of disinformation, dude.
“The most useful metric would be a statistically significant increase in total “All Causes” daily or weekly deaths. For the countries for which that kind of data is available, there has been no such increase.”
Liar. Not sure why brazen and repeated lies about objective facts should be tolerated.
Aside from the H1N1 epidemic, which I remember as being traced to Mexico or Central America, every single major influenza epidemic in the last hundred-plus years has come out of China or Southeast Asia.
One theory for this phenomenon has been that the Chinese in rural areas tend to keep pigs and ducks close to home. Both animals are susceptible to the influenza virus and seem to incubate new strains that get across the species barrier. As China becomes more urban, this might fade as a source but nothing suggests that it is absent by now.
For example.
Help me understand. In the absence statistically significant and accurate testing for the virus, why wouldn’t total deaths minus accidents, homicides, and suicides be a useful measure? That is, has a country’s total death rate from diseases increased significantly?
We will not know the deaths above average for some time, perhaps not even a year. That will ultimately be number we want to see, but there isn’t much way to get at it at present. Perhaps some will reason that if C19 mostly just killed off people who were going to kick off in the next two years anyway, maybe we overreacted. Even if that were known to be the case I don’t think you could get many Americans to sign on for that. I may be wrong, there.
It is not a bad thing to remind people how bad the flu is, so that perhaps more people will get the yearly vaccines, even though they seem to be diminishing in effectiveness over time. However, comparing C19 to the flu does not work on many levels. It is much more easily contagious, spreading rapidly through a population. It may or may not be more fatal, but it does not look very different at this point. It is not an order of magnitude less or more fatal, I don’t think from what we can see. In-hospital treatment for the seriously ill goes on much, much longer with C19, tying up resources like ventilators, which is what cause hospitals to become overwhelmed. AS it is an ugly way to die likely affects us somewhat, but I don’t think that should count against us.
If distancing and washing are having the desired effect of reducing exposure and death, I don’t think it follows to say “see, it’s not that big a deal.”
One only has to look at what is happening in hospitals in Italy and Spain to see that this disease does not behave like the yearly flu. If the overall death rate were similar to a normal year in the hotspots there there wouldn’t be people dying in the waiting rooms and parking lots. The Chinese, not known for deep affection for their everyday citizens might have just let things ride, especially as it’s largely older people who can’t fight back. They didn’t. No one who is near the disease seems to be treating it as small potatoes. That would be the people who are distant.
C19 does cause permanent lung damage in some who recover. Those years of life and years of health would also have to be factored into the final numbers.
Lastly, these deaths are in addition to the flu, not replacing them.
The second derivative is negative. This is rate if change of first derivative.
CR: That number is available for many areas, and I have linked to it. The lie is that those numbers don’t show increases currently going on. Where the data is available, they do.
Brian shouted “j’accuse”: “Liar. Not sure why brazen and repeated lies about objective facts should be tolerated.”
If you are going to accuse people of being liars, Brian, then you need to be able to back up that accusation with those objective facts.
At the risk of being repetitive, here are some of the limited sources of objective data available:
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/weeklyprovisionalfiguresondeathsregisteredinenglandandwales
All Causes deaths in England & Wales through 13-March: 11,019
Average deaths over the previous 5 years: 11,205.
Despite Covid-19, deaths are running below average.
https://www.euromomo.eu/
European wide data. No Covid-19 upkick in deaths compared to prior years.
As CapitalistRoader says, it would be good to see more granularity in the data, and look only at disease-related deaths. But if we really have a pandemic that is killing people in large numbers, we would definitely see it in the total number.
We need to be careful about analyzing the data. Italy, for example, made the bureaucratic decision that the death of an 85-year old man with lung disease, heart disease, and cancer will be counted as a Covid-19 death if he tests positive for the virus. Even Dr. Neil Ferguson from Imperial College, London whose models did so much to scare the politicians has since told Parliament that most of the people who die with Covid-19 in their systems would have died anyway in the next 2 or 3 months.
Brian, I don’t know about you, but my mind is open. I am influenced by the data, and I put low weight on model predictions and panicking media. Give me the objective facts. Show me the bodies!
The flu vaccine is prepared a year in advance and the Australian experience during their winter gives us some indication about how effective it will be. The flu strains vary year to year and the vaccine has to match well, which was apparently not the case this past season. Even so, the death rate may include some who would have died of flu mixed in with the WeFlu.
The present WuFlu seems to be a variant of the SARS virus and we don’t know if it will be seasonal yet. SARS and MERS are not but may be too virulent to be a good parasite and that may limit contagion.
AVI: “We will not know the deaths above average for some time, perhaps not even a year.”
How are we able to know the number of people who die with Covid-19 the very same day it happens — but will not be able to know total deaths on that day for a year or more?
Certainly, the media and the bureaucracy are not putting out the data on total deaths with the intensity & zeal they devote to reporting deaths of people with Covid-19. That may be a tell.
I commend Mark Steyn’s current reading of Daniel Defoe’s book about the 1665 Plague Year in London. The very first indication people had about the coming plague was a sharp increase in the daily number of people being buried. The limited data we have today does not show such an increase.
This question is important, because we are all paying a very heavy price for shutting down the economy over Covid-19, and we will all continue to pay that price for many years. We need to know what we are paying for.
Gavin: I already posted links in previous threads. Your ignoring them doesn’t change the facts, nor does it give me the responsibility to keep posting them. Go find them yourself, liar. Under my own name. From a few days ago. Your job to go fetch them.
Its just beginning. You have done little to mitigate its spread and Dr Fauci is very probably right that 100,000 Americans will die. I came to this conclusion a week ago. That’s probably a minimum and only if you practice social distancing and best practices religiously.
The video of the Spanish doctor crying his eyes out, as he tells us about his day spent pulling ventilators out of 65+ people, and putting them into younger people, is where your country is going.
Please take this seriously. Please.
Brian, who accuses others of being liars, ducked & weaved: “Gavin: I already posted links in previous threads.”
Sure, Brian. If you have objective facts, put them on the table. Or sacrifice your credibility.
It seems to me that determining a death is far easier than pin pointing the cause, especially in cases of multiple or shared causes. If we could in virtually real time know the daily death count that stat is the best indication of the true death toll of some new cause or the net difference from all causes in a particular year or season.
The issue of overwhelming our health care capacity is a key issue regardless of the mortality rate.
The issue of targeting prevention (including isolation) for the most vulnerable groups rather than massive shut down is another issue that needs more consideration.
Brian, you really need to cut the snark. It reduces your credibility as a serious person with thoughts worth considering. Being wrong is often distinguished from lying. Do you really think you can read the motives of others?
Death6
One caveat that I would keep in mind is that the derivative here is sensitive to time skew. Any change in the interval between cases being diagnosed and their posting would cause significant discrepancies. Ideally, you would have a time series where each test result was accompanied by the time that it occurred. Since results are presumably coming from many more sources now, the change in velocity could be from delays in posting. This should even out over time. I’m sure Professor Prost is far more aware of all the pitfalls than I am.
By the way, the second derivative would be acceleration.
The buildings that most of us work in have fire sprinklers. The installation and maintenance cost over the life of the building is significant. Most will never be used yet the money spent is not considered wasted because long experience has allowed us to determine that the loss without them would be greater.
Right now, we are in the position of ants climbing a hill. We probably won’t know when we reach the top and will only be able to tell in retrospect.
We’ll only be able to evaluate the precautions we’re taking now after this is over and then there will be no end to argument.
One way of telling the crypto-totalitarian is by how fast he writes off other people for the good of society.
Suicides will probably go up. Homicides–I don’t know. Accidental deaths, especially from car accidents, will drop dramatically. Those causes have to be removed for death rate data to have any meaning.
I can’t help but think those data are available close to real time for developed countries, somewhere.
AVI: Perhaps some will reason that if C19 mostly just killed off people who were going to kick off in the next two years anyway, maybe we overreacted. Even if that were known to be the case I don’t think you could get many Americans to sign on for that. I may be wrong, there.
I think you are right and that many Americans will not go along with utilitarian decisions by govts to trade the premature deaths by Coronavirus of individuals who are statistically likely to die within a few years, against the greater availability of treatment for younger people. For very old people, of whom there are now many, and their families, a year or five of additional life is of great value regardless of what anyone else thinks. Triage of the old vs. the young as a first resort seems like an artifact of socialized medicine. Perhaps Americans will spend, research and produce our way out of this problem as we have many others.
As of right now, I’m seeing total reported deaths 36,226.
Obviously that is tiny compared to the total number of deaths since the virus was first detected. Roughly 4-5 million people die per month.
But that doesn’t tell us anything about how many people are going to die.
Triage of the old vs. the young as a first resort seems like an artifact of socialized medicine. Perhaps Americans will spend, research and produce our way out of this problem as we have many others.
I think we are starting to see the effect of older people self isolating.
For example, new cases in Tennessee are occurring in those under 60.
Look at the age range in that bar graph.
Tucson, a city of 520,000, has 119 cases and 5 deaths. The area is home to many “snowbirds” who are retirement age. Even so, half the deaths seem to be in people of moderate age with pre-existing conditions.
Coronavirus has claimed a fifth life in Pima County, county health officials said Saturday.
The man, who was between the age of 18 and 40, was in hospice care, the county news release said. No further information was released.
Officials reported two deaths Friday afternoon, which was an increase from two on Thursday.
The first reported death was a 54-year-old Tucson woman on March 23 followed by a man in his 70s on Thursday.
Both had health conditions that may have put them at higher risk, officials said.
The health department then announced a man and a woman, both in their 80s, died from the disease.
So, two were in the advanced age group.
Gavin: You are a liar and a fraud. This is the last time I will ever respond to you. I had stopped doing so after you clearly and repeatedly demonstrated how unserious you are, and made a huge mistake in this thread of trying to engage you, but now that I’ve started I will show what a pathetic hack you are:
In this post at 9:56 on March 26, I included a link to a source discussing all source deaths for Italy:
https://chicagoboyz.net/archives/62251.html#comment-1031737
The link is here:
https://pandemic.substack.com/p/the-elephant-in-the-room-undercounting
At 10:02, you posted this, asking about All Source deaths:
https://chicagoboyz.net/archives/62251.html#comment-1031738
At 10:10 I posted this, pointing out that my link had just addressed that issue:
https://chicagoboyz.net/archives/62251.html#comment-1031739
And I included this quote, since you are unwilling/unable to follow links.
“[H]ere is the most important data point: in Bergamo, people are dying at 14 times the rate of a normal year. In the 8th-16th of March period, 330 deaths in 2020 vs 23 in the same period in 2019.
The essay contains other data points regarding the cities I managed to find the data online: in total, 6 towns in Northern Italy registered a total of 613 deaths over the last ~3 weeks compared to 73 over the same period last year: 8.4 times as much!”
On March 28 at 11:05 you posted this, claiming all source deaths show no increase:
https://chicagoboyz.net/archives/62257.html#comment-1031937
At 12:35 I posted this in response, pointing out that your claim is wrong, as I had previously already shown:
https://chicagoboyz.net/archives/62257.html#comment-1031948
And now today you bring up the same false claim, and when called on it (again), ask me to provide evidence, when you’re already demonstrated an unwillingness or inability to engage with any evidence that shows that this isn’t JTF, as you have insisted from the very beginning.
I don’t know or care if you’re a liar, a fraud, a troll, or just an unserious person with terrible reading comprehension skills, but you are not worth engaging with. Have a nice life.
“@Kirk – “My guess is that if we hadn’t had all the publicity, the entire “pandemic” would have vanished into the background noise as part of the annual flu season, and we’d have written it off as a particularly bad one–Until someone went back and did the work to determine what made it so bad.” I have been pounding the table on this point from the very start and agree 100%.”
Sigh. Go here:
https://a816-health.nyc.gov/hdi/epiquery/visualizations?PageType=ps&PopulationSource=Syndromic
These are NYC ER visits, by day, for a variety of causes.
No interpretation, no spin, just plain old numbers.
Plot the “respiratory” numbers, or ILI if you prefer, and aggregate by day.
You will see that this was a moderately severe flu season, and was basically over by the start of March, at which point the numbers start to skyrocket in ways not previously seen in the dataset. This doesn’t require some esoteric modelling to tease out. If MSNBC was still shrieking about whatever they used to shriek about, the plain numbers would still be undeniable.
Let me say that I think Gavin is mistaken but I don’t think he is a liar.
Hugh Montgomery of the Institute for Human Health at University College, London, says it is well established that those with the flu will infect 1.3, 1.4 others. The current estimate for C19 is 3 per person. By the magic of compound interest, that means 14 people after ten iterations for the former, 59,000 for the latter. I have seen smaller numbers, such as 2.5 per person, but it is still a big deal down the road.
Also, Italy and Spain are lowball numbers. They admit they are not counting those who die at home or in nursing homes, because there is just too much going on. Those countries which have slowed the deaths – as in the OP or your example of UK – may be the best examples to look at for what will happen in the US, which is following similar protocols, but I think is emphatically not the best data to look at for what would happen if we had had not “paid a heavy price for shutting down the economy,” as you remind us. I don’t want to be unsympathetic to those who are now in a bad place economically because of the government restriction on activity. But we have not “shut down the economy.” In this discussion at least, you are consistently overestimating the economic damage and underestimating the mortality. People do that to be dramatic and make a point, but I try to push back against such advocacy versus exploration.
I made other points in my previous comment which remain unanswered. I understand that the direct attack on your character by Brian attracts more of your attention, yet I will persist in following my own threads.
Here we are again. I am lucky enough to be heading out to work in a few minutes. I could spend my remaining waking hours scouring the internet for horror stories, which would likely increase my proportion of waking hours. Instead, I actively ignore them because they make no difference to what I need to do and I don’t revel in needless pain.
Doctors are notoriously bad a predicting who will die and especially when. As far as I know, no one is recommending taking living patients off of vents to use them for others here. It would violate all sorts of laws. I doubt that the differential between the age groups once mechanical ventilation becomes necessary are that clear cut. It seems all of the socialized medicine advocates have been selecting who to throw overboard for a long time. This is apparently too good a crisis to go to waste.
So, Brian who ducks & weaves, you have put forward a total on one (1) post by a certain Lucca Dellanna linking to another essay, also by her, noting increased deaths in a small region of Italy.
https://pandemic.substack.com/p/the-elephant-in-the-room-undercounting
You have not put forward any objective data supporting Ms. Dellana’s contention. Nor have you put forward any objective data covering a wider population, and you have not put forward any official data — certainly nothing comparable to the England & Wales data set showing the absence (so far) of any uptick in total deaths.
Any textbook on statistics will tell you about the tails of distributions. There is a psychological process called “confirmation bias”, where people seize on one piece of evidence from the tail of a distribution which supports their pre-existing conclusion and ignore much larger bodies of evidence that contradict it.
It is easier for someone to falsely accuse others of being liars than it is for that person to look objectively at a body of evidence which does not fit his preconceived ideas.
AVI: “Lastly, these deaths are in addition to the flu, not replacing them.”
Could you please expand on that statement. The data seem fairly definitive that Covid-19 leads to death mainly in the elderly and those with pre-existing medical problems (two groups which overlap substantially). That would seem to imply that anyone who is already suffering seriously from the flu (like the 390,000 people in the US already hospitalized with the flu this season) would be at risk of also being attacked by Covid-19. Why would there not be an overlap between people who die from the flu (22,000 in the US already this flu season) and those who die with Covid-19 in their systems?
Hey Penny: Apparently you actually are one of the more sane ones around here, who knew? FYI, I assume you’re not gloating about Mother Russia’s performance in this anymore. Vlad’s not walking around in a biohazard suit and locking down their major cities just for fun, you know.
Actually, he quite possibly is, ha ha.
How many ER visits are happening because of the publicity alone, Brian? How many people are there who would have shrugged this off as a particularly nasty cold, self-treated, and only gone in for care when crisis came… But, now that the COVID-19 panic-mongers like you have frightened them, they’re suddenly wanting care?
When all this is over, the people stoking fear and panic are going to be studiously ignoring what they’ve said, and will be denying that they ever spread fear, uncertainty, and doubt.
https://spectator.us/understand-report-figures-covid-deaths/
The key metric here is the question of how many have had COVID-19, right along the entirely subjective question of “How many have died with COVID-19 infections, as opposed to of COVID-19…”.
Both of those numbers are essentially unknowable. The data coming out of China is useless and entirely untrustworthy. The data here in the West is questionable, because we don’t even know what we don’t know, i.e., the prevalence of the disease in the population. Given the unfettered access we gave China to the world before President Trump shut down travel with China, odds are quite good that the COVID-19 virus has been here in the US long enough to become spread throughout the population already. Until they start sampling for the antigens, presuming that they remain in the victim, we’re never going to know.
Flatly put, the biggest thing about this self-inflicted crisis is that it is exposing the inadequacy of our preparations for these things, and the essential idiocy of engaging with any communist or socialist government in the way we have with China. Given their behavior, we need to tote up what this has cost us in economic terms, subtract that from what debt of ours they’ve bought up, and then isolate them again from the world economy until they stop lying about every thing under the sun. The state of the Chinese banking world is such that it makes their response to this pandemic look like a minor contretemps, and I would not put it past the Chinese kleptocracy to have taken advantage of this situation in order to crash the world’s economy to cover up the BS in their banking system. We still don’t know the real death toll from Wuhan, and that’s ridiculous. If the Chinese want to participate in the world economy freely and openly, then they need to behave as trustworthy participants. This incident shows just how untrustworthy they really are, and we need to cut ties with them until they can act like responsible adults instead of furtive little creeps hiding their problems from the world.
Kirk: I don’t know what to say. I show you objective numbers and you basically say it’s all just mass hysteria. At least you don’t try to deny they’re real numbers, like other JTFers, so that’s a step up I guess.
Are you ‘effing serious, Brian? “Objective” numbers? You haven’t quoted a damn thing that’s “objective” in any sense whatsoever.
All of the numbers are sheer fantasy, at this point. We don’t know the key metric, which is “How many have been infected”, and that’s because we don’t have testing that shows that. We have “People who’ve been tested because they showed signs/symptoms” and “People who’ve died with COVID-19”. We don’t really know whether those people would have died anyway, now do we? There is such a thing as comorbidity when it comes to disease, and the fact is, most of what we’re attributing to COVID-19 in terms of deaths are potentially entirely wrong.
A good illustration of the question can be found here, taken from CDC data:
https://accordingtohoyt.com/2020/03/27/covid-19-and-us-mortality-by-i-ratel/
Note the interesting fact that this year’s flu season fatalities are well below normal, per their tracking data. What the hell does this show, assuming that the CDC data are accurate?
Right now there are no numbers that are at all reliable for much of anything. We don’t know why, for example, that it some 85% of the people aboard the quarantined cruise liner in Japan remain asymptomatic. Nor do we have an explanation for why it is that the crew remaining in Japan with the boat aren’t all dying in job lots–I’ve yet to find anyone who is even looking at that metric.
Let’s face the facts: NOBODY has good numbers at the moment, and we’re not going to get them until we are able to determine just who has had the disease already, and suffered no ill effects beyond those of a bad cold or flu. From what I can tell from those CDC numbers, either this year’s flu epidemic is seriously weird, or their data reporting is woefully in error. My best guess is that we may even find out that this year’s flu deaths wind up being low enough to make the combined COVID-19 and flu totals come in below what were expected just for flu, this year.
On the other hand, we may all die when the bug mutates again and turns into something really nasty. Could be the Chinese engineered the perfect bioweapon, and we’re playing right into their hands.
At the moment, however, the only thing we can really say is that we don’t know what we don’t know, and none of the numbers make a damn bit of sense. China has lied from the beginning of all this, which is highly suspicious. Their actions since the beginning of it all are highly irresponsible, and are deserving of both censure and retribution. Which I am sure they will receive.
Brian, there’s nothing you can do. A closed mind must open its self. It is amazing that people in the face of quite obvious facts, are still in denial. Does anyone really think that America, can escape what is happening everywhere else?
@ Gavin – I have seen lists of what are considered pre-existing, and none of them have included influenza. It does make abundant sense that it might be on such lists, but I don’t see that it is. The conditions on the lists are stuff like kidney or GI disease, diabetes, heart conditions, obesity, hypertension, etc – Chronic rather than acute conditions. There are millions of those, so whatever the number of current flu sufferers is it might not even register on the lists.
Get off your high horse, Pen. Canada’s confirmed case fatality rate is 1.23%, the United States’ 1.93%.
Does anyone really think that Canada, can escape what is happening everywhere else?
AVI — Thanks for the explanation. It seems to be another example of us not finding what we are not looking for.
At the level of viruses, it is inconceivable that a flu virus and a Covid-19 virus shake hands and agree — you take the one on the right and I’ll take the one on the left. However, at the level of the harried medical professional, it is quite conceivable that she has to tick either the flu box or the Covid box.
No-one would want to suggest that having the flu protects a person from Covid-19 — or equally that Covid-19 protects a person from flu.
Kirk: My apologies for suggesting you are more reasonable than other JTFers.
We might expect the Canadians to escape significant illness caused death if a) it is their engineered bioweapon in the first place b) they carefully timed the release of an infectious counter agent to inoculate the Canadian population while leaving the US population vulnerable.
I) I’m not sure they could pull that timing off II) They’d be crazy to try, whether using an infectious counter agent, or one secretly distributed.
If it was unknown whether China was playing around with samples from your labs, would you really want to show a wildly better death rate than your neighbor’s?
I sort of scrolled past the argument. Anyone who takes anything Pengun posts as serious is making a mistake.
The best analysis is based on the cruise ship in which 20% were infected and 8 died. I expect this will be roughly the US experience once testing has caught up and we see the real CFR.
Meanwhile, my wife and I self isolate but not extremely. I went to the hardware store today for a bird block.
How does the NYC situation-population, density, international visitors-distort the USA statistics? I was a middle school English teacher and do not have a math background.
Mike K,
I don’t see testing “Catching up” in the USA without a major breakthrough in testing technology or a massive shift in US medical liability laws. Some of the new tests the FDA rush-approved -might- do that, if they do not have to use a skilled Medical Laboratory Scientist.
This is from my wife’s Facebook feed and it explains America’s COVID-19 testing shortage.
https://www.facebook.com/photo.php?fbid=10219999857820257&set=a.2780855374030&type=3&theater
In the United States right now, there are approximately 310,000 laboratory professionals employed. There are 2.89 million nurses employed. There are 1.2 million doctors. In the US, there are approximately 350 million citizens. For laboratory professionals who take the brunt of all tests, that leaves 1129 people per one laboratory scientist, and one person averages 39 various tests per year.
Right now, in this pandemic, we are at a shortage for testing supplies. This is something many media sources are reporting daily, and leads us all to believe that the biggest hindrance to testing volume in the US directly hinges on the availability of testing supplies… But this is not the only hindrance, and perhaps it is time to shine light on another hidden shortcoming in this country.
We are at a severe shortage of testing professionals, and we have been for many years. Our profession is one that tends to hide in the background despite our integral roles in disease research, patient care, treatment, and diagnoses… and this is because we tend to be the introverts or the nerds of healthcare, and we like it this way. Most other healthcare professionals don’t even realize we require 5-7 years of college education.
Last week, in a 6 day period, the US performed 335,000 COVID-19/SARS2 tests. At the time, there were 62 labs capable of performing this testing. Each test takes approximately 15 minutes of hands-on time, and these 62 labs employ approximately 1600 lab scientists. This means 83,750 hours of testing occurred across 1600 people. To accomplish this, each scientist would have required 52 hours to accomplish this volume ON TOP of all the other testing that is required because other diseases don’t stop because of a pandemic due to a single virus. And this is all assuming none of these professionals get sick.
We are at a severe shortage of testing supplies, yes. But for too many years now, we have also been at a critical shortage of the only professionals capable and trained to run these tests for the 3rd largest population in the world.
Short Form: The effing American medical legal liability culture demands super educated Medical Laboratory Scientists rather than med-tech’s in testing companies, corporate hospital administrators won’t pay for robust innate capability with lessor trained people in hospitals for cost & liability reasons, and public health has been a playground for incompetent SJW for flipping decades with little or no testing capacity at all.
And now COVID-19 has near maxed out the US testing capacity at 300K a week, while Germany is doing 500K on a much smaller population.
#headdesk.
Pengun,
Regards this:
>> A closed mind must open its self. It is amazing that people in the face of quite obvious facts, are still in denial. Does anyone really think that America, can escape what is happening everywhere else?
Yes, very much so.
Pandemics are tests of adaptability for individuals, institutions and cultures.
Many are utterly incapable of believing in the changed Pandemic reality without personally suffering pain and the emotional loss of people close to them.
As my Grandma Dora used to say, “Those who cannot see will be made to feel.”
Trent, this latest test system looks like it is automated.
When I attended medical school, back when dinosaurs roamed the earth, we took a course in laboratory medicine. That is no long part of the curriculum at the medical school where I taught until 5 years ago. Neither is bacteriology.
Medical students no longer dissect a cadaver and anatomy is pretty much a skim over the details. Lots of stuff on feelings, though.
Let us hope so Trent. I want to leave a quote from a great American, which pertains to the ability we have to access information so easily:
“Information is not knowledge.
Knowledge is not wisdom.
Wisdom is not truth.
Truth is not beauty.
Beauty is not love.
Love is not music.
Music is THE BEST.”
Frank Zappa
Egad. Frank me no Zappas. Possibly the best example of pseudointellectual to come out of 60s rock.
I admit the competition is fierce, there. I think I will write a post on that soon.
I posted the instructions that the CDC was sending to the labs for the test that was current at the time. There are other test now that use different instruments and different protocols but I’m sure that outside of slight differences in details that they will look similar. It even included how to program the instrument.
Once you penetrate the jargon, you see a very mechanistic series of instructions, not that different from a cooking recipe. It requires meticulous technique and access to special facilities like bio-hazard vent hoods and of course the instruments to process and then analyze the samples. None of this requires profound understanding of chemistry, molecular biology or any ability beyond following instructions and procedures accurately and consistently. I don’t imagine that anybody here couldn’t perform adequately with a few hours of training and that would mostly be in proper technique and not at all about the underlying science.
Developing the framework that the test is based on and to a somewhat lesser extent applying it to this particular virus did require high level knowledge and expertise. Running and controlling the lab require high level knowledge as well.
There is no reason that a lack of people to physically manipulate the samples should be a bottleneck. There is no difference between this test and any other that a lab performs. They are required to train, supervise and confirm the accuracy of the techs, the instruments, the reagents and the procedures used. A much more likely problem is physical space and special facilities. Preventing cross contamination for tests that detect nanograms or picograms of material requires physical separation.
I doubt that many if any of the actual techs has much beyond a B.S. and probably not much more recourse to their training on a day to day basis than the average barista.
“Possibly the best example of pseudointellectual to come out of 60s rock.” LOL. A genius and very great musician is a pseudo intellectual? Methinks you are not paying enough attention, or perhaps your various prejudices are showing themselves here.
This appears to be the antibody test and is automated.
It will not be useful for detecting newly infected cases but will help with learning who is immune and can leave quarantine.
I think it makes good sense to ignore PenGun.
Hi Mike. A Fugue for you: https://www.youtube.com/watch?v=3r8a7HnnjTs&list=OLAK5uy_mfxKPK6xP1jAzLFyd7S-N6KZFzU6KQqEg&index=33&t=0s
Perhaps we should look to the future.
China is the world leader in creating new and wonderful virus variants in their rice paddies. The birds from East Asia then party in Siberia and Alaska, etc. All the birds return South in Fall or late Summer.
Most of the “interesting” virus out-breaks in the last century have appeared in the territory under major migration flyways. MERS (2012+) in the Mid-East, COVID-19 (2019) in Iran, the current chicken Corona virus in Israel. The Spanish Flu (1918) in Europe and Kansas. The recent Flu outbreak in Central America.
Maybe we should be paying attention to the bird migrations. That might allow some time to prepare. Ever the optimist, COVID-19 may just be the first wave to get to the West. If Corona-SARS is seasonal, some lead time would help.
Trick question? The JH curve doesn’t look like that. I think the runup in testing also makes it hard to interpret the numbers during the middle of March. Frankly, it looks like that last point in the cases curve was from before the number stabilizes in the evening.
The problem with the data is that it is meaningless as far as tracking the progress of the epidemic. The title should read: “Number of Confirmed Cases that Somehow manged to Receive a Test while we were desperately trying to test as few people as we could get away with”
You can draw any conclusion you like and so can I. Each would have some small chance of being right. I like to compare those sorts of numbers with the chance that either Harry or I will become King of England. Mine is exactly zero, his; so very little larger as to be essentially the same. So we’d both have Harry’s chance.
MCS,
I may not count as ‘here’, but I bet I would not perform adequately as a tester, even if trained. I have issues with dexterity, and paying attention. I suspect this is similar to other activities that I’ve not practiced to excellence. I get bored and stop paying attention to what is happening, or I get impatient, and make stupid choices when trying to decide what to do next. It is possible that I would have become competent if I had opted to continue investing the time, but I’ve long felt I would be better off spending my time on stuff that won’t suffer if I forget what is going on, and isn’t very fragile.
That said, I can believe that there are much more than half a million people in the US who could do a good job with those tasks.
re: excess deaths, more statistics starting to be compiled and released from European countries. Outlook: seriously undercounted, and grim.
https://twitter.com/bastiaan_brak/status/1245999935130140672
Statistics Netherlands (CBS) reporting excess mortality attr. to #COVIDー19 for 16-22 March in excess of 500 compared to same period in 2019.
Official death toll related to Coronavirus over same period *only* 233.
-> substantial ‘hidden mortality’ in NL
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3567093
Combining official statistics, retrospective data and original data (i.e., obituaries and death notices) we provide a tentative estimate of the “real” number of deaths caused by COVID-19 as well as the total number of persons infected. Our findings suggest that the reported mortality rate attributable to COVID-19 accounts only for 26.6% of the observed excess mortality rate between March 2020 and March 2019.
Similar compiled numbers from France, Spain, at least, also available.
Brian — Thanks for posting the link to that SSRN article. It is good to see actual data.
The article reports some staggering numbers — this year in certain municipalities in the Lombardy region of Italy, 8,560 total deaths were recorded in March, versus only 3,504 total deaths in March last year. When the number of deaths more than double, something is certainly happening!
If this doubling of total deaths was happening everywhere that C-19 has been identified, there would be no debate about the seriousness of the infection. But data from other places, such as the UK, show essentially no increase in total deaths. What is happening?
If we dig into the SSRN article, the authors state that they selected 434 municipalities out of the 1,506 municipalities in Lombardy. The authors chose those particular municipalities because they were showing increased mortality compared with 2015-2019. In other words, the authors are looking only at data from places where the death rate went up — not for all of Lombardy.
Why did recorded deaths go up in about one quarter of Lombardy municipalities? Perhaps those are the municipalities where the major hospitals are located? The data may be showing a change in procedure — instead of people dying at home or at a local hospital, those suspected of having C-19 are sent to the major hospitals where, after treatment, they die. Thus there could be a concentration of deaths in certain municipalities.
Of course, that is mere speculation. But we know for sure that total deaths in European countries are not spiking. Another factor the SSRN data confirms is that Covid-19 deaths are rare for people younger than 65, and are mostly concentrated in people over 75. These are the people whom Imperial College’s Ferguson said were likely to have died in a few months anyway regardless of C-19.
This raises a very difficult moral question — how much of a burden is it fair to impose on children, students, working age people in order to extend the lives of the very old by a few months?
This year and maybe next year there will surely be excess deaths. But the following years there will be a deficit in deaths, as many of the infirm and soon to die, will have already died.
I wonder what %age of those deaths will occur in older folks suffering from something like Alzheimer’s? Both my mother, at age 83, and my father, at age 91 passed away 2 years apart.
Both of a wasting disease. My 2 older sisters tended for them for 6 years each- 8 years in all. When they both were admitted to an extended care facility, my sisters would tend to them morning, noon
and supper time, every day. Had they passed on a year or 2 earlier, I know for certain, that it would have been a blessing for all concerned. The young will pay a very heavy price for this compassion for the old.
Raymondshaw: “This year and maybe next year there will surely be excess deaths.”
That is what the Powers That Be would certainly like us to think — but they are not putting any data on the table to support that.
Data on C-19 deaths is questionable because of co-morbidity; and it is subject to being massaged by bureaucrats. The most trustworthy numbers are Total Deaths from All Causes, which should be much higher than normal if we are in a real pandemic — but, surprise!, those numbers are hard to find. They are available for England & Wales — remember, England is the place where the Prime Minister is reported to be infected with C-19. And the English data are showing fewer Total Deaths than normal, probably because of a generally mild flu season.
But don’t take anyone’s word for it. And for sure don’t believe anything you see in the media. Look at the data for yourself.
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/weeklyprovisionalfiguresondeathsregisteredinenglandandwales
Gavin, here is the logic behind my remark. I am 68 YO with several of the so-call co-morbidities often mentioned. I believe the actuarial tables give me a life expectancy of 15-16 more years to enjoy my retirement. But, let’s say this coming Christmas season, I catch this virus and perish on Dec. 31. That would be an excess death. But happily, I won’t die later on, which would make me a deficit death for some future year.
I am more on the What, me worry? side of the spectrum rather than the Chicken Little sort.
When I was driving to work, I noticed a anti drunk driving billboard. Probably a lot less of that now and fewer traffic deaths in general. That’s roughly a hundred a day normally. With hospitals really paying attention to infection and most elective surgeries canceled, there will be fewer deaths from iatrogenic causes. That’s supposed to be 80-90,000 a year.
Am I the only one that finds all of the so called ethicists disturbing when they get up and seem to assume that we will finally take them seriously and let them decide who will live or die? They seem to rubbing their hands together at the prospect being able to finally set an age cutoff for ventilators.
Of course the hallmark of a free society is individuals making decisions for themselves. It is a constant war between those that want to be free and those that either know better or want some sort of guaranty of “security”.
Anonymous (Raymondshaw)?) wrote: “let’s say this coming Christmas season, I catch this virus and perish on Dec. 31. That would be an excess death.”
Not necessarily. Statistics cannot make a prediction about any particular individual; statistics can make predictions only about very large groups.
The actuarial tables say that a large group of 68 year old men with your health conditions will on average live for another 15 years, until they are on average 83 years old. But if you look at the data on which those tables are based, some men die at 68 (sorry!) and some men live until they are 99.
If you (a particular individual) die this December, that will be sad — but it will not necessarily be an “excess death”.
This year, statistics predict that about 2.9 Million of us in the US will die — averaging about 7,800 every day — from all kinds of causes. (Top 3 are heart disease, cancer, and accidents; flu is #8 on the CDC’s hit parade). Fearless Fauci says that 200,000 of us will die from C-19. If at the end of 2020, it turns out that 3.1 Million of us have died, then Fauci will have been proven correct. There will have been “excess deaths” due to the virus.
If at the end of 2020, it turns out that 2.9 Million of us have died, and frantic Fauci is still claiming that 200,000 died from C-19, then we will know that there have been no “excess deaths”, and instead the bureaucrats are simply relabeling the reported cause of death.
If I die from one thing rather than from another thing, that is not relabeling the reported cause of death, it is a different cause of death.
My personal opinion is that we will see considerably fewer Covid 19 deaths than the lower estimate (100,000) given by the good bureaucrat, but we shall see.
Doctors learned, approximately 2,000 years ago, to NEVER give an optimistic prognosis. If the patient died, it was always to be expected. If the patient lived it was evidence of the skill of the doctor.
That is Medical School 101, taught in the first hour of the first day.
The CDC is only following that thousand year old rule. Of course the death toll will be less than projected. I expect it will end up close to a bad flu season and the CDC will take credit.
The economic consequences will be none of their doing. They don’t do economics.
Seriously, we have to start opening up the economy after Easter, which should be the peak of the epidemic. Hydroxychloroquine will affect the results.
My wife takes HCQ for rheumatoid arthritis. I have read somewhere that no patient taking the 300 mg per day does has been diagnosed with COVID 19. They, of course, are the more susceptible population as almost all are older and impaired.
Mike K I think you are correct.
Those of us who are Star Trek nerds like to call that the “Scotty Principle”.
In business we call it “Under Promise & Over Deliver”.
Raymondshaw: “My personal opinion is that we will see considerably fewer Covid 19 deaths than the lower estimate (100,000) given by the good bureaucrat, but we shall see.”
We are basically on the same page. By that, I mean that total All Causes deaths in the US this year will not be much different from the 2.9 Million last year.
However, we also have to recognize that the bureaucrats control the words written on death certificates. If they decide (as per Italy & UK) that any hint of C-19 gets a death listed as caused by C-19, then the number of deaths ascribed to C-19 could get rather large. 100,000 people die in the US in less than 2 weeks. That is why only the total All Causes deaths are a meaningful guide to the scale of this asserted “pandemic”.