Note: The graphs in this post may require an administrator to be made visible, which I have requested. In the meantime, those graphs and more are at the link. (I take it back. It looks like they came up first time!)
I wrote early on that there would be errors in both directions in the Covid count of deaths, that some might be called C19 that could be better attributable to another condition, and some ascribed to flu or pneumonia that were really coronavirus. A couple of months ago, when the drumbeat started that there were all sorts of deaths being called Covid that really should be called something else, I repeated that claim of errors in both directions, but noted that our numbers were more likely an undercount than an overcount, largely because some places require a confirmed diagnosis of C19 before it can be put down as a cause of death. This was unpopular in some corners. As reports of more suicides crept into the news, more attributable to lockdowns than to other explanations (isolation, loss of employment, anxiety) I likewise cautioned again: wait for the data. Do not speculate on why something has happened until you know that it has actually happened.
Please note, this is true for other countries as well. Everyone seems to have excess deaths, and it is difficult to measure how many at present. There are different problems in counting in rural vs urban areas.
I think it is now fair to say that the C19 deaths officially reported are a severe underestimate, not an exaggeration. The numbers from this Lyman Stone thread are pretty devastating in that regard. The excess deaths from all causes are in tandem with Covid spikes and recedings, not lockdowns. That is, where there are more C19 deaths, there are more excess deaths as well. This doesn’t leave a lot of room that they could be anything other than unrecorded Covid. The exception is “external causes,” which would include homicides, suicides, drug OD. Those are down, not up, though there may be some change in those numbers as more complete reporting becomes available. But there would have to be lot to move that red line above the covid line.
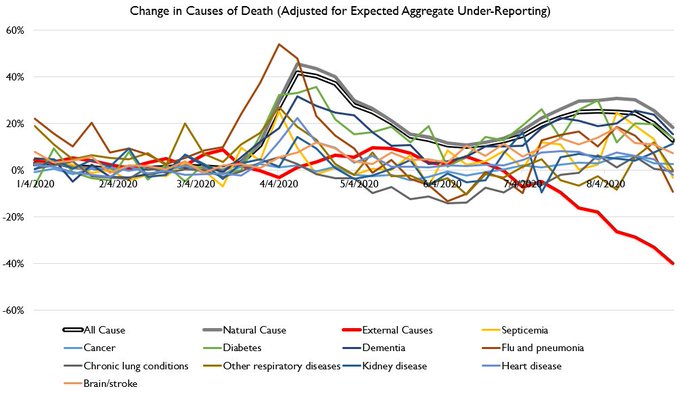
Some of the excess deaths are likely attributable to care for other conditions that was not given, either because the medical providers discouraged it or the patient thought they should not go in. Yet again, these graph lines track Covid deaths, not the shutdowns that would have created the other conditions. Many areas changed their rules for hospital and clinic admissions long before they have very many cases. I don’t see that in those colored lines above. If there were a lot of that, it would show at least a little. Similarly with the next graph:
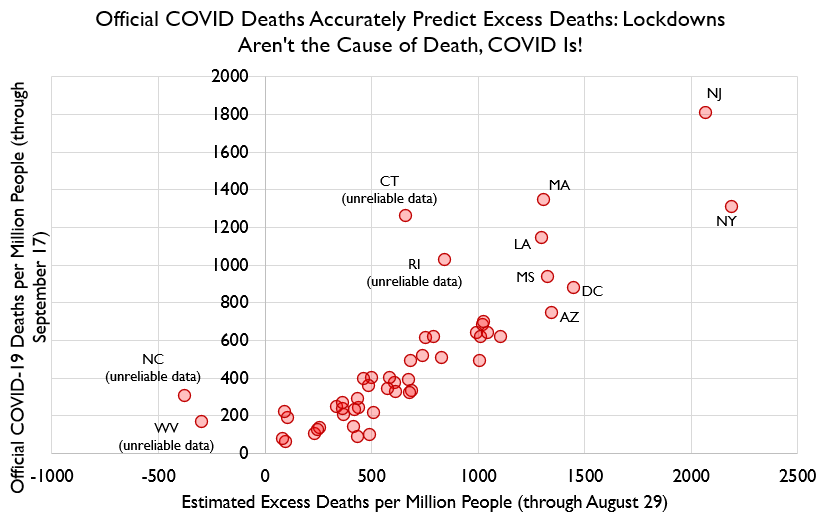
That’s a very tight pattern. To quote Stone from the link, who is pretty emphatic “Excess deaths spike when covid deaths spike, they spike where covid deaths spike, and the residual of excess minus official covid deaths is ALSO correlated with covid deaths. In other words, excess deaths are covid deaths.”
I have read a fair bit of speculation why the coronavirus numbers must be inflated, that hospitals get more money for that, that they are under political pressure to make C19 look bad, or that they are calling everyone with covid who dies a covid death, etc. Except that all falls apart if the numbers aren’t actually inflated. It is a bit of reasoning I learned from CS Lewis decades ago: there should be no speculating and explaining of why something happened until we have established that the think has actually happened. (I will note a parallel in the discussion of systemic racism. First demonstrate that this occurs before engaging in lengthy speculation why it occurs and why people don’t want to hear it.) As the old joke about the hasenpfeffer recipe goes, First, catch a rabbit.
For now, deaths from external causes are not up, they are down. But deaths from everything else are up, with no ready explanation other than they are actually unrecorded coronavirus deaths.
If it’s any comfort it seems that other countries numbers are even less accurate than ours. How high? If you follow Stone’s thread, it might be as much as double, though that is the high estimate.
The initial comparison to flu deaths was so dumb in part because flu deaths are a statistical estimate, and covid deaths were trying to count confirmed cases. Excess deaths was always the obvious way they should be, and will be, estimated.
I just this evening on twitter saw a plot claiming that excess deaths are now back to “normal” finally.
I have to say that unless you are going out and conducting actual confirmation tests on every death, most of this stuff is not that far removed from random number generation.
Case in point–Relative of mine was found dead on the 12th of September. Last time anyone saw them alive was around the 26th of August (some argument between witnesses as to when they were seen). What’s on the death certificate? Died on the 12th, supposedly, even though the mortuary was virtually certain they’d been dead for at least two weeks due to the state of the decomp. Cause of death? The doctor put down cardiovascular disease, but it could have been any number of other issues they were undergoing treatment for. They just made a guess at it all, because there’s no way in hell that anyone could have performed an autopsy to figure it out, with the body being as far gone as it was.
The data itself is only as good as the people filling out the forms and submitting it. How much of it is guesswork and supposition in the first damn place? You can project a certain degree of certainty about it all, based on statistical confirmation, but do we really know what the actual numbers are, vs. just being representative of what’s the currently popular best guess by the various involved data-gatherers?
It all looks logical and sensible, right up until you go out and actually look at how this information is being gathered in the first place. Factor in the number of false positives and false negatives generated by the various different tests, and you have to seriously consider the possibility that the whole thing is an exercise in fantasy.
Has anyone gone out and tried to do a sample survey, and actually verify these things by double-checking the inputs? That’s always my issue with all this statistical work–You should be able to see where there’s been a reproducible sample verification in the data, and you never, ever see such a thing. At least, in any of the various studies that I’ve been able to actually dig into the data with. A lot of the time, with public health issues particularly, it’s all like Michael Mann’s infamous “Hockey Stick”–The whole thing turns on some black box in the numbers that they don’t show the data or the algorithm it was all based on.
Off-topic anecdote – not data-driven – but human nature:
My mother died at 79 in 1997; my brother was irritated that the young emt man had declared “cause of death” as “from old age.” She was in retired housing but not assisted living and had died of a heart attack – apparently – about 16 hours before her neighbor got the door opened, worried because they usually shared morning coffee. At the reception after her funeral, one of her friends, in her nineties, consoled me, “it was sad” mother “had died so young.” My idea of “dying young” has slowly aged as I have. Nonetheless, she had given a weaving demonstration the afternoon before, gone out to a card party that night, and died during the night. Statistics that rely on such casual analysis of “cause” must not be terribly meaningful, but in the midst of Covid probably higher standards prevail.
Thanks for your clarity & myth-busting; I’d certainly assumed that the extra govern-ment money for covid had influenced the numbers. I guess I should have been more optimistic about human nature.
Seems to get back to the philosophy of causation. If a person has severe cardiac disease and dies “with” a Corona Virus infection, what is the actual cause of death? The virus is deadly to those with co-morbidities, so the virus might be expected to harm/kill more of those who are vulnerable, hence “excess deaths” from all “causes”. This possible change in attribution, across the board, suggests that the criteria for “cause of death” aren’t very helpful, especially with a disorder like COVID-19 which may damage vascular function in the entire body in addition to the obvious “lung mung”.
And what are “natural causes”, in this context? How might those be aggravated by an infection and the resulting fatigue or unsteadiness? What is the ultimate “cause”, say death from a blow to the head from a fall due to unsteadiness during an infection?
“Excess Deaths” with COVID-19 doesn’t seem to tell us much beyond, “disease kills the weak”.
The Economist has a project to measure excess deaths in a wide range of countries and US states, most recent update was 8/28.
https://www.economist.com/graphic-detail/2020/07/15/tracking-covid-19-excess-deaths-across-countries?utm_campaign=coronavirus-special-edition&utm_medium=newsletter&utm_source=salesforce-marketing-cloud&utm_term=2020-07-18&utm_content=cover_text_url_3
There are many situations in which a death has events/conditions in the chain of causation. For example, a nurse gives a patient, who is a child, a dose of medicine which is much too large. But the pills of the different dose levels look exactly the same, as do the bottles they come in. If the bottles or pills had been visually distinguished, then the nurse’s error would probably not have occurred.
Another example: an airline flight crew entered the wrong destination code into the navigation system (this was before the days when moving-map GPS became commons) and commanded the autopilot to fly straight to that point. The autopilot obeyed perfectly, right into a mountain.
The cause of the accident was in one sense the flight crew’s error by not properly entering and verifying the code: but if the nav system’s designers had provided a display that showed even the first few characters of the selected destination’s name, then the error would almost certainly have been caught.
Probably the most useful way of defining a (direct) Covid-19 death would be one that would not have occurred at that time or within a very short interval around that time (say, a couple of weeks) had the patient not been infected. An indirect Covid-19 death is one that would not have occurred had not the the *society* been infected, even though the patient himself was not. (missed treatments for other conditions, ‘deaths of despair’, etc)
The point of the post is that “cause of death” as listed on a death certificate is wholly irrelevant. We know COVID was a huge killer, and posterity will know, because there was a massive spike in deaths over historical levels that lasted for ~6 months (it seems for now to be almost gone in many places, is my understanding), and unless you can come up with another answer, it’s covid. It’s an aggregate argument, not an individual case argument.
And yes, it will be quite interesting to see how “excess deaths” look this winter, and next year.
I am also in the camp that excess deaths are the only ones that matter in this context, the assigned “COVID” number merely serving as a proxy. Part of this is because of limitations in the reporting system (the CDC’s weekly track of deaths has a built in 10 day lag in reporting anything, and the last two month’s worth of data needs significant adjustments to estimate as yet unreported deaths due to delayed reporting). It’s bad enough that death lags infection by 2 weeks, throw in another 10 days and you are talking about a month’s lag in getting data, which is clearly not actionable in any practical way. The whole system is riddled with estimates because you have policy makers trying to make decisions in real time, or even in anticipation of future infections, while the most valid number you can work from won’t be available for a month or more.
BTW – the latest weekly update is due to be released today. Last week’s report (for week ending Sept 5) was the first since the epidemic broke to be below the excess threshold (although the prior week was only just over the line). If this week is also below (again, these are still estimates) then that would suggest pretty strongly the epidemic has largely passed (as of a month or so ago). It passed months ago in the parts of the country hit strongest in the initial outbreak, as those areas have been showing normal deaths all summer. Now its passed in the southern states that saw a summer outbreak. Assuming this holds up, I don’t think we will see the data show an excess between now and December (historically most excess death periods occur during flu season anyway.
Hmmm. It was a couple of months ago I told you, on your site, that the excess deaths everywhere, were judged by some to be pretty well all C19. You could go look at that, and see if you were somehow influenced by my post. Gotta be careful, lies are everywhere, and who knows what evil one might ascribe to, by mistake. ;)
Or, PenGun, we can continue to ignore your dumb comments per usual.
The most interesting thing in the excess death data for me is the age distribution. Basically there are no excess deaths in the under 25 cohorts, rising to about 10% (of normal death rates) excess between there and the 55 & over groups. Because deaths are normally heavily skewed to the older populations anyway, this means the increased risk (of death anyway) for the working age population in aggregate is minimal (in absolute terms). It is this distribution that drives most of the observed variability in CFR – it’s not the disease or response that’s influencing the CFR, but differences in which parts of the population are coming down with it. Some of that may have stemmed from policy (in the US, the decision in a number of states to push recovering COVID patients back into nursing homes is a fairly obvious mistake in retrospect, there were some analogous decisions made in Italy as well). So while I still think our understanding of the dynamics of the spread of the disease is incomplete, our understanding of who the disease actually kills is pretty solid.
Have not yet studied this in any depth, but looks interesting. It is about the dangers of false positives in testing.
https://lockdownsceptics.org/lies-damned-lies-and-health-statistics-the-deadly-danger-of-false-positives/
I’m probably being too sanguine but it would be more alarming to me if he found large gaps in excess deaths that *didn’t* correlate to COVID. At least we can assume we are getting the directionality of the trends right if not the absolute numbers.
“the decision in a number of states to push recovering COVID patients back into nursing homes is a fairly obvious mistake in retrospect”
Not just in retrospect, but at the time, it was completely and totally obvious. I pointed out here repeatedly (I don’t have the energy to find it specifically) the fact that the nursing home in Washington which had one of the first outbreaks in the country had something like 30+ deaths in a few weeks, compared to an average toll of a few per month. That was way before Cuomo ordered nursing homes in NY to take covid positive patients. The only very slight defense would be that they were desperate to keep hospital beds clear for the building number of patients from the general public, but to claim that it wasn’t know that that would cause catastrophe is revisionist history. It is a tragedy that our contemporary world is so hopelessly partisan, and that this happened during an election year.
Statistics are always interesting and informative, but… The question should always be asked “Where do these numbers come from?”. In this case, we’ve got a very stressed system generating them, and a lot of pressure to lay blame on Covid.
I’ve been talking to a couple of people who work with the homeless. For whatever reason, they’re telling me that they see limited to no impact that they can identify as being Covid-related deaths in that population–Which you would intuitively think would be horribly vulnerable to it. Why aren’t we seeing that, and why aren’t the homeless shelters and campsites inundated with dead bodies of victims?
There’s another effect from Covid, too–How many people have gotten sick with something else, something they would have normally ignored until it got bad enough to kill them, but with Covid on their minds, they’re going straight to the doctor in fear they’ve gotten it, and instead get life-saving treatment for what they do have?
I think we really need to be looking at the entire population here, not just the ones that are sick and who die. What’s out there incubating in the general population, at the moment? Additionally, the question ought to be asked and worked on is what Covid might be setting us up for in the future. One of the things I remember reading about with regards to the 1918 flu epidemic is that there had been another, earlier epidemic back during the 1890s which seemed to influence the mortality rates during the 1918 outbreak:
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0069586
Age-Specific Mortality During the 1918 Influenza Pandemic: Unravelling the Mystery of High Young Adult Mortality
The worldwide spread of a novel influenza A (H1N1) virus in 2009 showed that influenza remains a significant health threat, even for individuals in the prime of life. This paper focuses on the unusually high young adult mortality observed during the Spanish flu pandemic of 1918. Using historical records from Canada and the U.S., we report a peak of mortality at the exact age of 28 during the pandemic and argue that this increased mortality resulted from an early life exposure to influenza during the previous Russian flu pandemic of 1889–90. We posit that in specific instances, development of immunological memory to an influenza virus strain in early life may lead to a dysregulated immune response to antigenically novel strains encountered in later life, thereby increasing the risk of death. Exposure during critical periods of development could also create holes in the T cell repertoire and impair fetal maturation in general, thereby increasing mortality from infectious diseases later in life. Knowledge of the age-pattern of susceptibility to mortality from influenza could improve crisis management during future influenza pandemics.
Obvious issues:
no chart for what the lockdown status was at that point, which means there is no evidence offered in relation to lockdown status
no attempt to compare when non-emergency-medical was shut down to spike in deaths (a specific aspect of lockdown)
only mention of non-disease lockdown deaths is in terms of external causes such as suicide, even though stress causing a much higher rate of heart attacks has been well known for decades now
https://www.webmd.com/balance/news/20031112/heart-attacks-spiked-nyc-after-9-11#1
and further study has identified that being socially isolated is correlated with a nearly 40% higher risk of heart attack, stroke, or other major cardiovascular event; Takotsubo syndrome or “broken heart syndrome” is not that obscure.
chart for changes in cause of death by more specific causes starts in January, which is a severe lack of context– which really should’ve jumped out to both him and anybody reading since “flu and pneumonia” starts out at 20% over normal, and “other respiratory diseases” is nearly there. Has the data somewhere, since cumulated deviation from excess deaths starts in October
Under 18 deaths being down– motor vehicle deaths are generally a huge chunk of under 18 deaths, if not THE biggest killer. Of course those deaths are down when people are under house arrest, same reason that my insurance company has been refunding chunks of our premiums due to relatively few folks driving.
@ Pen Gun – yes, I get all my good ideas from you. I’m still sure there are going to be massive deaths from the superspreader Sturgis event you warned us about.
The Lyman Stone link goes to TWITTER, for Goodness Sake! One of the first rules of evidence is that anything on Twitter is probably a misunderstanding, a misrepresentation, or an outright falsehood. So I have not wasted any time on that.
Kirk is correct to enquire into the source of data. Another factor to consider is “excess” over what? Annual deaths per million population in the US have ranged from as low as 8,124 in 2008 to as high as 9,649 in 1950. That is nearly a 20% variation from low to high. https://www.macrotrends.net/countries/USA/united-states/death-rate
What do we take as the “base” over which “excess” is measured? Death rates are highly variable year to year, and there are hard to untangle trends due to changing demographics and medical changes.
This is a complicated topic — way beyond anything that can be analyzed appropriately on TWITTER !
“more attributable to lockdowns than to other explanations (isolation, loss of employment, anxiety) ”
Surely the latter, in this context at least, are a first-order result of the former.
Gavin-
Yeah, the “our theory says X would have died normally, but Y died, so it’s from this cause” has been objected to in calculating flu deaths for several years now. It’s a house of cards built using a tool that is supposed to be comparing before and after a change, not a seasonal event. At best you could do a yearly (or 5 year average?) baseline, which would of course have all causes of death wiggling up and down across the line because deaths do not happen at a steady pace, and much less are they reported at a steady pace.
Otherwise, you get whatever you tell your model it should expect.
I did click through, to see if the source was linked– but I also listened to guys on Coast to Coast AM to see if they gave sources for their claims, and found some good information that way, but it’s not the way to bet. :D
Source wasn’t even listed on the pictures– not even in the “I am hiding something” tell style of writing the .gov site it came from, rather than the specific report or page(s).
Which means the source for the statistics is, indeed, twitter. It’s sad that there were enough other serious issues that “there is no source for the data” didn’t have to be listed.
I don’t go on Twitter myself, and only encounter such things when someone sends them along. However, a fair number of very decent researchers put their stuff up on Twitter as part of open science. A number of major players in genetics research, for example. Lyman Stone is a legit researcher with significant scientific training. https://thefederalist.com/author/lyman-stone/
Folks would probably do better to look a little closer at what was actually up there rather than reflexively reject what goes against their own opinions.
Gavin is the equivalent of Penny on all things covid. Nothing new has come from him since early February or so. The notion that a plot showing how death rate has varied over time means that excess deaths are unable to be measured is kind of new and especially bizarre though.
Brian’s curious assertion: “… excess deaths are unable to be measured …”
That sounds like an attempt to distract from your own earlier erroneous “sky is falling” claims about how bad Covid-19 was going to be, Brian. You were wrong then — get over it! There is no disgrace in being wrong; we all have to make judgments based on incomplete information. There is disgrace in not being able to admit that one was wrong.
As for your silly claim, no-one has ever asserted that “excess” deaths cannot be measured. But the question of what is the baseline that they are being measured against is a valid one — one that the Twitterati seem unable or unwilling to address.
LOL, show me where I made wrong claims that you’re referring to, Mr. “Just the flu”. You are so certain, I’m sure you have the evidence right at hand. Oh wait, you can’t because, as always, you’re a liar.
Brian demeaned himself: “… you can’t because, as always, you’re a liar.”
That is an Ad Hominem, Brian. Almost as bad as using Twitter as a reference. It means you have no argument — no factual basis for your earlier claims that Covid-19 was going to be a medical disaster.
The facts have not changed significantly since the early results from the Diamond Princess. The vast majority of the population either don’t catch Covid-19 (maybe many of us are already resistant?), or if they do catch it, the symptoms are very mild. The small At Risk minority are those who are very old and/or have serious pre-existing conditions. About 1 person in 1,000 in the general population will die with/from Covid-19. Not exactly a pandemic.
Those who are pushing Project Fear are talking up a storm about the expanding number of “cases”. But they have deliberately changed the definition of “case”. A true medical case is a person with signs & symptoms of a specific disease, i.e. a sick person. Project Fear “cases” are people who test positive for the presence of a piece of RNA or an antibody — most of whom have no signs or symptoms, i.e., they are not sick. There is ever-expanding testing for these “cases”, and the low percentage of positive test results is suspiciously close to a typical rate of False Positives in a well-run testing environment.
Now, Brian, you can stomp your feet and claim that all of those factual observations are “lies”. But all you would be doing is embarrassing yourself.
My apologies to ChicagoBoyz readers for being so direct, but honestly Brian you should not demean yourself by descending to unsubstantiated Ad Hominems.
He’s an agricultural economists. In cotton. Who use to work for the USDA, trying to figure out world demand, and worked in “tax policy” before that.
That does not make unsourced charts which have the long list of basic problems I pointed out any more legitimate; in fact, it makes it so that he should know how to show proper evidence and deal with very basic scientific literacy problems like this, if he is engaging in science.
Heck, if he is based in rational persuasion, he should be giving context, and sources. The only thing his background shows is that he should know all the problems I pointed out. And yet, he published them.
If he is engaged in rhetoric, then it’s appeal to authority, which is not a form of rational persuasion.
As a follow-up, the latest CDC excess numbers are out and they have basically shifted the end of the curve a week forward (numbers from 2 weeks ago are now modestly above the excess threshold, last week has moved slightly above the threshold, and this week is again well below), so the only rational conclusion is that they don’t have the adjustment factors tuned quite right and there is still an underprojection of excess deaths in the short term. So we continue to experience above normal deaths from all causes, and we’re not out of the woods yet.
To Brian’s response to my nursing home point above – I prefer not to call decisions made in a situation of great uncertainty as clear mistakes at the time. From what I can see, those decisions were made in the face of projections of a rapid overloading of the health care system and were made knowing that this would cause deaths in nursing homes, but in the belief that it would save more lives by avoiding the “collapse” being seen in Italian hospitals then. I have no idea what constraints existed in nursing homes in those areas, so while I can imagine other options (moving patients to create “COVID-only” homes would be the obvious one) I have no idea if they would have been practical. American politics being what they are, none of the governors involved would actually admit this is what they were doing publicly, but I’m comfortable making the inference. There were seven (at least that’s the number in my head) governors who made this decision, and this would be the obvious common thought process.
I didn’t agree with the decision either, but then I didn’t bear any responsibility, so that’s easy for me to say.
“From what I can see, those decisions were made in the face of projections of a rapid overloading of the health care system and were made knowing that this would cause deaths in nursing homes, but in the belief that it would save more lives by avoiding the “collapse” being seen in Italian hospitals then.”
There was a hospital ship..retrofitted to be able to handle Covid cases…available and not being used. Ditto for the hospital capabilities that had been built out in the Javits Center.
Not just in retrospect, but at the time, it was completely and totally obvious.
I’d just like to note that sending infected patients into nursing homes was so obviously a mistake that the chief Pennsylvania state health bureaucrat pulled his mother out of a nursing home before ordering
it to be done.
You don’t do something like that if you think everything is going to be just fine, in my view.
Paul-
it’s pre-emptive triage with known fatal results.
That is, they did something they knew would result in deaths, because models that had not been accurate in any time or place they’d been tested said there would be a flood of people.
Even then, since all elective medical care was shut down, they could have set up actual quarantine wards.
But.
That would remove the justification for whole-population “quarantine.”
It would also be expensive.
…kind of like that population that was killed by the policy.
Funny, isn’t it, how if they’d been practicing eugenics and death-panels, they wouldn’t have needed to change a single reaction?
Also, note, they did not stop the order when it became clear that there was no overwhelming surge coming.
In an inexcusably evil move, NY also just passed a law making it easier to sue nursing homes for not protecting their patients against covid. You know, those patients that the state ordered them to take.
OK, correct me if I’m wrong, but…
50% of all CV deaths are and have been consistently those 75y+… this is from CDC figures.
The Life Expectancy in the USA is currently 78.5 years. It actually varies from 74.8 (WVa) to 82.3(HI)
Life expectancy is the median age of death in a population group… like US residents.
So, in reality, Covid is not even really killing anyone all that earlier — for the most part, it is merely “the bullet that got you” at the end of your life.
This suggests that the majority of the concern over CV is hysteria, not actually reasonable fear.
I suppose you might make an argument based on an undemonstrated narrowing of the normal curve of age at death, but that seems about it…
78.5 is the current approximate life expectancy at birth.
The current life expectancy at age 75 is around 12. See https://www.ssa.gov/oact/STATS/table4c6.html.
A disease-induced culling of the elderly population is hugely costly in the aggregate, and of course for the individuals who lose their last 1, 5, 10, 20 years. The aggregate cost only appears low in comparison with that of an epidemic that kills mainly younger people, such as the Spanish Flu, but that’s not the best comparison to make.
Thanks Jonathan – that is the kind of thing I tend to forget and therefore not think this through in a proper way.
I do think that there is something especially scary about the death of young children (as polio often caused) and I do think that while those of us in our mid-70’s on can live productive lives, bringing happiness to others. However, I have had a shot – something a 30 year old hasn’t – at doing what I wanted to do in the lifetime I’ve been given.
I do love Fogel’s optimism that describes what we consider average height and health as “stunted” and average age at death as “premature.”
Over on RedState, there’s an article about Doctors who came out against the lockdown, and the more than 600 who signed a letter back in May decrying the inevitable results of the lockdown:
It is impossible to overstate the short, medium, and long-term harm to people’s health with a continued shutdown. Losing a job is one of life’s most stressful events, and the effect on a persons health is not lessened because it also has happened to 30 million other people. Keeping schools and universities closed is incalculably detrimental for children, teenagers, and young adults for decades to come. The millions of casualties of a continued shutdown will be hiding in plain sight, but they will be called alcoholism, homelessness, suicide, heart attack, stroke, or kidney failure. In youths it will be called financial instability, unemployment, despair, drug addiction, unplanned pregnancies, poverty, and abuse.
https://www.redstate.com/michael_thau/2020/07/13/many-medical-experts-were-against-lockdowns-the-media-just-didnt-want-us-know/
I have to wonder, here, how much this applies to “excess deaths”, as opposed to CV19. It’s nontrivial as at least a question as many of the fatalities are older victims, who may be lacking some cognitive function, and also wonder why their loved ones haven’t been there to see them in months. People do die of “broken hearts”, and this can include older people who miss their family. Moreover, even if you eliminate suicides directly, you can’t attest to how many strokes, heart attacks, and other systemic failures can be attributed to loneliness, depression, etc., inducing these. These factors can be contributing even if they don’t lead to overt negative actions.
Again — not saying I know the answer — but it does offer what, to me, is a legitimate alternative answer to the argument of “excess deaths are covid deaths” that is AVI’s treatise, and which needs to somehow be considered and eliminated before accepting his Null Hypothesis…