“We should act incrementally as prudent risk minimizers and pursue any effective no-regrets options. We do not have to wait for the formulation and acceptance of grand strategies, for the emergence of global consensual understanding, or for the universal adoption of more rational approaches.”
— Vaclav Smil (Global Catastrophes and Trends: the Next Fifty Years)
This post is an attempt at synthesis; those just grazing in (Midwesterners don’t surf) are directed to Reopening — I (Practice) and Reopening — II (Theory) for accounts of my earlier action and contemplation, respectively. For my third installment, I can do no better than lead off with a quadrant diagram of my own devising:
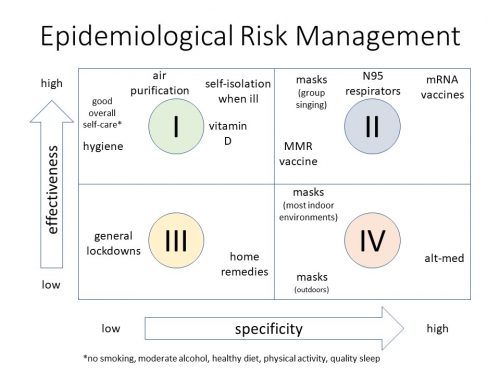
The above came to me after realizing that the so-called NPIs (non-pharmaceutical interventions) so widely recommended to fight COVID-19 were, at least by contrast with a well-targeted vaccine for SARS-CoV-2, relatively non-specific. So I decided to make “specificity” the independent variable, which puts it on the x-axis, and the obvious dependent variable f(x) would be effectiveness, on the y-axis … and recall from Taleb that unless you have the luxury of doing pure research, you need to concentrate on f(x). To a good first approximation, then, the general population should be adopting, or avidly pursuing, the things in quadrants I and II, and ignoring—in some cases simply violating—the contents of quadrants III and IV.
Priorities readily emerge from this analysis …
Conceptual
- A subtle but desperately necessary point is that individual differences must be respected, individual perceptions of risk in particular. “Then lest us stop judging each other; rather, use your judgment to keep from offending your brother or putting a stumbling block in his way.” (Romans 14:13, Lattimore)
- Low-specificity, high-effectiveness tactics should be strongly preferred, for their versatility in managing future incidents (about which more in the next entry in this series). They are not necessarily cheaper from the perspective of an individual consumer or employee, but their yield across decades and generations is unsurpassed.
- High-specificity, high-effectiveness tactics are, by definition, relatively unique, but include the gold standard of a well-targeted vaccine, which is vitally necessary in environments otherwise lacking in institutional functionality and financial margin, which is to say the Third World (and marginalized locales in wealthier nations).
- Everything else. Individual experimentation should of course be allowed, but quadrant III and IV tactics—very much including general-population lockdowns—should not be imposed as a matter of law, except perhaps as a very local response on the scale of a neighborhood or a small town.
Concrete
- Air purification is quite simply the single best institutional response to this pathogen (and many others). Libertarian though I am, I would seriously consider advocating requiring that all new construction include it and that all existing public accommodations retrofit it within the next few years. Its hierarchy of effectiveness looks like this:
- Dilution ventilation with outdoor air, basically running HVAC blowers continuously—and/or opening windows, wherever possible—for more air changes per hour (ACH); 4.5 ACH gives 90% relative risk reduction, and 6 ACH = 95%. A more strictly quantified recommendation is 7-10 L sâ» ¹ persâ» ¹. In the case of the venue I’ve helped, the total volume of air in the auditorium is ≈9 × 10âµ L, and a reasonable maximum number of people present simultaneously is 100. At 10 L sâ» ¹ persâ» ¹, that’s 4 ACH. The total cross-sectional area of the supply ducts is ≈0.5 m ², requiring air movement of only 2 m secâ» ¹ (≈ 4.5 mph) to meet the criterion. We are actually getting 6 ACH and thereby 95% protection from this technique alone. Not to overlook the obvious, outdoor events are essentially perfectly safe at anything like normal areal densities of crowds (~1 pers mâ» ²), even with almost no air movement. Also, “energy-efficient” buildings with no openable windows are more or less maladaptive.
- Inactivation of pathogens, usually with irradiation or reactive oxygen, possibly with humidification.
- Irradiation, specifically ultraviolet germicidal irradiation (UVGI), means UV-C, generally λ = 200-280nm, with peak effectiveness at λ = 265nm but most commonly in the form of bare (that is, no phosphor) mercury-vapor lamps at λ = 254nm. KrCl excimer lamps with λ = 222nm are becoming available. UVGI is phenomenally effective, sometimes reaching 20 ACH equivalent, but also phenomenally expensive, $~100 mâ» ². Hospitals and some other very high-traffic facilities use it, but they have large budgets. The very good news is that this will be largely meliorated, starting as early as next year, with the ramp-up of production of UV-C LED germicidal lamps with λ = 265-280nm. I expect not only lots of these to be mounted inside HVAC ducts but to be widely used in the form of “puck lights” for surface decontamination, especially in kitchens and bathrooms.
- This is just to separately note that UV-B (λ = 280-320nm) is only ~20% as effective as peak UV-C, but it’s a lot better than nothing, and it’s free in the form of sunlight. One more reason to do things outdoors and/or open windows whenever possible.
- Reactive oxygen species-based techniques, in the order of familiarity to me: bipolar ionization, dry hydrogen peroxide (DHP), and photocatalytic oxidation (PCO). Bipolar ionization as installed in the venue where I have assisted is providing an additional ~80% protection, taking our 95% risk reduction from 6 ACH up to 99%; it is also currently about an order of magnitude cheaper than UVGI. DHP has an if-you-have-to-ask-you-can’t-afford it quality, seemingly suitable only for very large, high-traffic buildings. PCO is of imprecisely determined but probably significant effectiveness against viruses; its cost appears to be greater than that of bipolar ionization but less than UVGI or DHP.
- Humidification is of lesser, and variable, effectiveness but I again note that it often comes free with outdoor air, so get outside or open those windows!
- Filtration is being communicated as a simple matter of upgrading to MERV 13 or higher filters to trap more virus. MERV is an acronym for Minimum Efficiency Reporting Value; MERV 13 filters will capture nearly half of flu virions and reduce relative risk (RR) of infection to 64% of its baseline, unmanaged value, even in the absence of any other measures. They will also, however, substantially increase the static pressure load on HVAC systems. Some large fraction of existing installations will be damaged over time by reflexively installing these filters. (HVAC is going to be a very good business to be in for the foreseeable future.) In the effort I helped manage, our decision was to upgrade from MERV 7 to MERV 10, which gives us an RR of 72%—and in combination with always-on HVAC and bipolar ionization, pushes our overall risk below 1% of what it would be with no mitigation at all.
- Vitamin D supplementation is supported by numerous studies finding that likelihood of developing a severe, or even noticeable, case of COVID-19 plummets as blood concentrations of vitamin D rise above 30 ng mLâ» ¹.
- Darker-skinned people, elderly shut-ins, and most of the population in wintertime are susceptible to deficiency due to lack of UV-B sunlight, less efficient synthesis in the lower layers of skin epidermis, or both. This is a significant element in the present growth of case counts, with increases in severe cases at the margin and attendant drawdown of medical resources. I remain astonished that supplementation is not receiving greater emphasis by public-health authorities, especially since most blacks and Hispanics in the US are at least borderline deficient.
- Essentially everyone in the population should take 4000 IU (100 mcg) of vitamin D₃ per day, and many people should take 10,000 IU (250 mcg). Toxicity does not begin until far above this level, probably 30-40,000 IU per day, and this vitamin has numerous health benefits. Minority residents of Kansas City are at around triple the risk of death from COVID-19 of the general population, and the age distribution nationwide notoriously skews older, to the point that nearly half of all deaths have been in nursing homes.
- The combination of better ventilation/air purification and vitamin D supplementation alone would almost certainly drive the Râ‚€ value of SARS-CoV-2 below 1 and snuff the disease out in a couple of months. The messaging on this has been as fragmentary and inept as the vaccine development in Project Warp Speed has been focused and successful.
- Masks don’t work well in many of the environments in which they are “required,” but there are a relative handful of situations where they are highly effective, and in those situations, failing to require them is seriously negligent.
- As noted above, outdoor air provides so much protection that with the possible exception of mosh-pit-level density, say 2.5 pers mâ» ², combined with lots of talking, shouting, or singing, there’s no point in wearing masks outside.
- Most office environments are low-density, ≤0.1 pers mâ» ², and mask-wearing offers only about 90% RR. Grocery stores appear similar; I note that 2-meter spacing = 0.25 pers mâ» ², and stores are rarely if ever so crowded (nor are the customers talking with one another in large groups, much less singing or shouting). And their HVAC is certainly running nonstop.
- Properly worn N95 respirators are far more effective, providing 10% RR, but they are relatively uncommon, and very few people are adequately trained in fitting them.
- Restaurants and entertainment venues with seating densities of ~1 pers mâ» ² should both address their ventilation and require masks whenever possible, by way of providing constructive alternatives to the disastrous policy of social distancing, which has devastated small businesses and caused a secondary pandemic of mental illness. We should pretty much be willing to wear moon suits to get rid of social distancing.
- The issue for churches is similar, especially for group singing; measurements of hymn-singing with and without masks indicate a reduction of over 90% in aerosol-droplet production, ie RR < 10%. Bluntly, any church not requiring masks is run by very careless people.
- Vaccines—and prioritization thereof—will be getting plenty of attention over the next few months. The success of Operation Warp Speed has been astonishing, and the new technologies utilizing mRNA are among the greatest blessings of our time (and accordingly are hysterically opposed by conspiracy theorists, but I’m saving a SWOT analysis of what project managers call “risk events,” both positive and negative, for my next post in this series).
- Front-line medical workers seem likely to get the first wave of available doses, which is as it should be, but I suspect that many medical people quite far from the front line of this struggle will also be included, and human nature being what it is, various ostensibly important or essential political figures as well.
- The next priority then ought to be the high-risk populations already mentioned: any combination of dark-skinned, elderly, the severely obese, those with histories of recent infections or major surgeries, etc. I am less confident that this will actually be done, and not at all confident that if done, it will be well-received. The list of what might be called Durkheimian sacralized entities in American society is not, to put it mildly, universally agreed upon. Giving the first available doses to, say, EMTs is one thing; moving somebody to near the front of the line because they have a BMI of 40 or compromised liver function from decades of alcohol abuse is something else, even if they are (say) a teacher in an inner-city school district. But this is another one for the SWOT analysis.
Bibliography of sources (other than my own experiences as recounted in the earlier entries in this series) I have found useful in compiling the above:
- https://www.nationalacademies.org/event/08-19-2020/federal-facilities-council-webinar-protecting-building-engineering-and-maintenance-staff-from-covid-19
- https://www.nationalacademies.org/event/10-28-2020/federal-facilities-council-webinar-heating-ventilation-and-air-conditioning-strategies-in-response-to-covid-19
- https://www.nucalgon.com/
- https://www.nfhs.org/media/4030003/aerosol-study-prelim-results-round-2-final.pdf
I’m confused: Does the RR number mean the risk reduction, or the remaining risk? You say that masks for hymn-singing reduce aerosol product by 90%, ie a RR<10%…which would imply that RR is the remaining risk, not the risk reduction…is that correct? 'RR' would also be an abbreviation for 'risk reduction', which is a term used elsewhere in the post.
N95 masks are not highly effective at reducing viral transmission … no study has ever shown that …
Jay, mega thanks for a well researched and well presented analysis. Just the sort of info I have been seeking. I’m sure there is more to say, but you have given some actionable info I believe I can trust.
Death6
I’m curious about your opinion on the value of masks. “…reduction of over 90% in aerosol-droplet production,”. I’ve read over and over again (just purchased “Unreported Truth’s About Covid-19 and Lockdowns”, Alex Berenson’s pamphlet that Amazon tried to censor, but have also read previous studies on NIH that no one pays attention to any longer) that masks are not effective in preventing the transmission of the virus. I won’t go into virus microns, droplets, filtration of material, etc., it’s all out there to read.
Is your opinion based on masks being effective in preventing viral transmission in restaurants and churches (especially the singing) based on scientific controlled studies? I can understand not wanting to sit in a restaurant or in a church pew or choir loft with people coughing and sneezing around me. In ordinary times it’s a bit annoying, if not repulsive, but according to so many experts masking does not prevent the virus sailing through the cloth or medical masks and into the air.
I don’t really know if masks are effective or not, but I do know that the vast, vast majority of people are not wearing the correct type of mask, nor are they trained how to wear a mask correctly. And it would be impossible to train everyone – a certain group of people are untrainable or unwilling, or have the inability to wear a mask (i.e. handicapped, senile, etc). In addition, when causally shopping or out and about, you see most people fidgeting with masks, speaking over them, wearing them improperly, and on and on. As I have said all along, if wearing a mask that may or may not be effective keeps everyone a bit calmer and keeps everything open, I won’t die on this hill.
Joan Anonymous,
Them thar’s figtin’ words. At least some places.
First, there’s this quaint concept of medical ethics that prevents placing a few thousand people in rooms with known concentrations of the virus and seeing who gets sick and comparing that with what sort of mask they were wearing.
That leaves retrospective studies that will all come down to wading through what people remember doing and wearing. I’ll make a bold prediction that when we are knee deep in these in a couple of years, you’ll be able to find studies to back any conclusion you can conceive. As far as anything now, not much and less you can trust.
From a purely mechanical perspective, the sort of masks that stand away from the face would seem better at protecting the wearer than those that lie against it like about 90+% of the non N95 masks out there. This assumes that a thin layer of filter material and a very few millimeters of moving air provides added protection from the the viruses that are presumably accumulated on the outside.
In terms of protecting others from the wearer, nearly any barrier would seem to offer protection from expelled droplets. The paradox is that the gross droplets that are best controlled have the least range, they fall out of the air quickly. It’s the small, invisible ones that float indefinitely, travel long distances and are most easily drawn deeply into the lungs. I can easily construct a mechanistic case that masks could enhance the production of these very small droplets. I can probably construct the opposite case as well. Plausibility is not fact.
Then there’s the real world where you have to consider people singing in a crowded choir loft or occupying a crowded public conveyance for long periods versus passing someone on a sidewalk and everything in between.
The idea of fitting an N95 mask is simply false, I am familiar with the process of fitting respirators for use where hazardous gasses are present, there is no way to do that with a disposable device. There is the process of putting them on properly that can make a difference, but if you look at the instructions, there will be a prominent statement that these are not to be used where there is an acute danger to human health.
Thanks for the responses. My exposition could have been clearer on a few points.
To clarify about risk reduction vs relative risk, they’re inversely related (and unfortunately could both be abbreviated RR, although the latter is the sense in which I used the abbreviation in the post).
The situation I’m helping out in may be characterized by:
(HVAC running a lot for 6 ACH) × (bipolar ionizers) × (MERV 10 filters) = 90% reduction × 80% reduction × 70% (to 1 sig fig) reduction = 0.1 × 0.2 × 0.7 ≤ 0.01
So, couple of orders of magnitude reduction. An obvious (to me) question is ”¦ why isn’t just that first 90% reduction good enough? My answer is that for a one-time event, it might be, but this is for, as it happens, every Sunday morning for months on end, and that 10% remaining risk starts to add up. I want two (or more) digits knocked off of this thing, not just one.
On masks, the challenge is, to borrow a phrase whose source I can’t recall, to find the grains of truth in the silo of nonsense. The closest thing to a blanket recommendation I have is:
1. wear one wherever anyone asks you to, simply to lower their anxiety (remember, the other pandemic is about mental health)
2. crowded indoor environments in general, especially if people are talking
3. group singing indoors is a must-have
4. outdoors, definitely not unless specifically asked
Specific to singing, I refer you to slide 18 from the final listing in my bibliography at the end of the post; the unit of measure is number of aerosol droplets per cubic centimeter.
I wore disposable surgical masks for 50 years in operating rooms. It was to reduce wound infections and I assume it helped. Viruses don’t cause wound infections.
Secondly, if any of you has ever had a joint replacement, the implant was done in a “laminar flow room.” That is because surgical masks are not effective enough. We are still talking about bacteria, not viruses.
I have a box of paper masks in the car and my wife and myself wear them when legally required to do so. The issue of the mental health of “Karen types” is the best argument I have read for using them.
I should add that the surgeons in the “laminar flow room” wear what we call “space suits” which resemble the astronaut suits that went to the Moon. The exhaled air goes out a tube and to the floor. And we are still talking about bacteria, not viruses.
Here is a article, briefly on the Johns-Hopkins web site, that seems to challenge the whole narrative. Taken down without an apparent explanation or retraction. I haven’t fully digested it but the webinar it is based on seems to propose that there have been no measurable excess deaths due to Covid-19.
https://notthebee.com/article/a-few-days-ago-johns-hopkins-published-a-study-saying-corona-is-nbd-they-then-deleted-it-read-it-here-in-its-entirety
Not a good way to reinforce credibility. The source seems to be something other than a scholarly paper but from a seemingly reputable person making a more or less public presentation.
Here’s a PDF of the original article:
https://behindtheblack.com/wp-content/uploads/2020/11/A-closer-look-at-U.S.-deaths-due-to-COVID-19.pdf
MCS and Jay,
Gosh, your replies/comments are both so calm regarding the masks. :) Quite refreshing, really. I understand the mental health aspect of people wearing the mask — how it makes some feel more secure in an unsecure world. I just hate seeing the children being forced to wear them. My grandchildren hate them — and they are required to wear the masks in order to go to school and attend any activities. I had to go pick up my middle grandchild a few weeks ago from school — her nose had been running (allergies), and she’d been to the office three times that morning to get a new mask (a cheap ‘medical’ mask). When I checked her out, she was wearing her own cloth mask that she’d worn to school that morning. It was pale blue material, and it was saturated with her mucous, the material that was wet had turned darker blue. Our older grandchild’s face started breaking out from irritation wearing her mask to school. I asked the youngest (still grade school) do you have to wear the mask all day long, and he said ‘we get breaks.’ :) I said, that’s nice. My sister had ordered me a face shield and I showed it to him. He now wears it in class. He wears a mask to school when we take him because he can’t walk in without one, wears the shield, and then wears his mask home on the bus. Yesterday I noticed a mask (smudged, dirty) on my husband’s center console in the car, and I asked him ‘whose mask is that?’ It was our grandson’s.
Yesterday out for a walk in the park (beautiful, breezy day, think high fifties, maybe low sixties) I was coming down a hill and turned onto the path that runs alongside a small lake and saw a couple with their young son. They all had masks on outside. It just puzzles me. I thought, ‘Why are they wearing masks outside? Don’t they read?’ I’ve gone to yoga and tai chi all summer long — outside at another small park. We don’t wear masks.
It just makes no sense to me.
“laminar flow room” – reynolds got your number
Joan Anonymous,
You neglected the group most comforted by the masks. That’s the politicians that can bask in the illusion that they are in control. If Trump had come out strongly for masks, we would all be going around with our bare faces hanging out.
For children it makes even less sense. They are at essentially zero risk and essentially zero risk of passing it on. They are appeasing the teachers. Just another example of the inversion that has taken place in public education where everything matters more than actually providing knowledge to the students.
Is the risk reduction benefit of MMR vaccination a relatively recent finding? If so, you apparently expect it will hold up. Is the benefit only in disease severity, or might it also confer some immunity from infection and/or reduce transmission?
Masks are useful, but its distance that matters. That seems to be almost completely ignored, not only in America but all over the world. Any crowd is spreading C19, while well spaced people, spread far less. That seems to be too much for most of humanity. This will not just go away, and is mutating, with rather scary results, in some places.
Human stupidity is our greatest problem, and this pandemic is highlighting that very well indeed.
Clif Guy,
It could easily be a false correlation. Via Wikipedia: “The MMR vaccine was developed by Maurice Hilleman.[3] It was licensed for use by Merck in 1971.[15] Stand-alone measles, mumps, and rubella vaccines had been previously licensed in 1963, 1967, and 1969 respectively.”
So if you were born much before ’71, you’re less likely to have gotten it, I know I didn’t, having already acquired immunity the old fashioned way. We know older = more risk for poor outcome so this may be nothing more than that.
I’m sure there are no shortage of people willing to theorize at great length. Just one more of those questions that may be settled definitively after it ceases to be a concern for most of us. Science may give us the answer but not when we really need it.
Clif Guy Says:
November 29th, 2020 at 12:42 am
Is the risk reduction benefit of MMR vaccination a relatively recent finding? If so, you apparently expect it will hold up. Is the benefit only in disease severity, or might it also confer some immunity from infection and/or reduce transmission?
Measles was a pretty severe disease. I had it and had to stay in my room with the lights out for a week. Most deaths, I think, were from encephalitis and that had a significant mortality, maybe 5%. In the Civil War, measles went through army camps like the Spanish Flu did in 1917, with about the same mortality. My great uncle, who was 18, got it and got encephalitis, which killed him about a year later.
Mumps causes sterility in adult males.
Rubella has a severe effect on fetuses in pregnant women. It was called “rubella syndrome.”
My kids got all the immunizations available at the time. They all got chicken pox as 2 year olds. My wife got chickenpox at age 16 and nearly died.
The real question is: Is this in the can’t hurt, might help category vis-a-vis covid?
I read through some of the information on PubMed about adult inoculation. It included statements about being able to prove that you had the various diseases. At this point, I have vague memories and, since my mother passed away many years ago, no real way to confirm them let alone some sort of proof. People born before 1957 are considered immune to measles and mumps which are included in my memories for what it’s worth and I am of that vintage. My medical consciousness wasn’t developed enough at the time to differentiate between measles and German measles. Then during the ’60s, there’s the question of just which sort of vaccine I might have received.
So the question remains, should all of us old farts heigh off to the nearest clinic to get a jab? There was little said about side effects and I believe it’s one of the cheaper ones as well.
Wolfgang Wodarg, a German Lungen Facharzt (Lung Dr.), who helped prevent a similar over reaction to the pig flu, believes the immunization (RNA) is terrible. He’s maligned by the mainstream media in Germany because he doesn’t follow along with what the government’s pro covid19 politics says. He says there will be little to no side effects directly following the injection. The problems will come later on – things like cancer, impotence, etc. But he believes one of the biggest problems is when the second immunization is taken – fall 2021 when the first is given in the next two months. He believes that about 300,000 people in Germany will die due to the second immunization. He’s also very skeptical of the genetic changes the immunization causes. All I’ve seen are German language videos of his.
As I understand it, the two doses are 30 days apart. Us proles will have plenty of time to gauge the side effects by the time they get around to us. Don’t know who the first doses will go to, probably health care as they should and other “essential” workers. Bet a lot of politicians will make the list. I plan to wait patiently before making up my mind.
One speculation I heard was that the vaccine will invalidate all the covid tests. Like I said, speculation. The problem is that all the erstwhile authoritative sources of information have badly overdrawn their credibility reserves. I’m counting on widespread problems being impossible to hide, we’ll have to see.
There are plenty of American crackpots with M.D.’s, don’t see that Germany should be any different.
For 1, in addition to vitamin D, consider Zinc as well. As I understand it, when therapies are applied, the presence of a suitable supply of zinc for the therapies to utilize assists in speeding their onset. Medical pros may differ, but that is what I’ve encountered, and my own GP concurred.
}}} I have a box of paper masks in the car and my wife and myself wear them when legally required to do so. The issue of the mental health of “Karen types” is the best argument I have read for using them.
Part of the question should be, however … should we be coddling the mental issues of Karens??
This is part and parcel of the whole “offensensitivity” problem becoming pandemic itself, today.
Neoneocon has an interesting piece on this…
…And why should the world protect you if you feel “unsafe” because of speech?
https://www.thenewneo.com/2020/11/28/and-why-should-the-world-protect-you-if-you-feel-unsafe-because-of-speech/
Surrendering to Karens is counter to the civilized tolerance of others. The general social sense of anxieties is to be accepted and given shrift, not the anxiety of its most extreme members.
Mind you, this isn’t a pronouncement on my part… I’m open to argument… but my own personal response/sense of direction says “that way lies madness“
Anon above is me… :-/
In defense of the zinc issue —
https://www.webmd.com/lung/news/20200923/could-zinc-help-fight-covid-19
They ack the above is inconclusive, but it’s clearly indicative, and falls into the “can’t hurt may help” arena… unless your doctor says you personally shouldn’t take Zinc, it’s probably a good idea to do so.
Because I don’t hate the Chinese, I have been following their advice since March. So I have Zinc as one of the 5 pills I eat every morning. I have been taking Vitamin D for a decade or so.
Fascinating, and I am going to go back and look at the whole series in order tonight. [stumbled on this via Assistant Village Idiot].
Your mitigation approach seems eminently sensible going forward.
I was struck by your comments on social distancing. I appreciate the economic catastrophe for restaurants, bars, and small retailers. But I am always surprised by the sheer amount of social and mental health damage being done, and the circumstances in which it is often reported.
I have had some advantages, though ones shared by a substantial minority of people- still had a job and income, was still actually doing it in part from home and in part from the office, could walk to and from in 45 minutes in spring and summer weather, and lived in a city in which no one was ever really forbidden to walk around outside, though some did choose to never do so based on their own risk assessment and variable quality official advice. So I had work, money, and purpose that many lacked. I had fresh air and exercise, available to all in my city who cared to go out in them and was not physically immobile. I always had access to grocery stores and pharmacies.
I do not fail to acknowledge these things, only note that where I live they were not a privileged I alone had. Also, masks required only from about May and only indoors in public accommodations. On-street is purely voluntary or habitual. I have no ailment that makes it in any way difficult to breathe through one. Though they all fit poorly.
All in all, not an especially demanding lockdown compared with those who got COVID, or got or had something else and had to await care, or who lost their jobs.
All down to temperament, I guess. I am going to come out of this pandemic, presuming it doesn’t kill me, remembering the number of people who found it deleterious to their mental health, even if they had jobs, income, food, shelter, and their health, just to have to keep 2 metres from people, or wear a mask, or forgo trips out of town or costly vacations or big family gatherings for one year.
I don’t mean that sarcastically, either, though I know it can appear so. I knew I was of a minority temperament, but I had no idea how much so. I have had some experiences with severe anxiety and depression, but this was not it. I will truly takeaway from this event a different appraisal of what is needful and what can or cannot be endured by a society and its members.
OBloodyHell,
I’m with you in being quite reluctant to go the way of a Karen’s Veto / paranoid’s veto on normal living.
Also like someone above, I only now discovered Parts I and II, and was fascinated by Jay’s generational observation. Here in Puget Sound Country it seems just the opposite: the old farts are disgruntled at the government overreaction; the young folks rush to see who can outdo Tsar Inslee’s decrees.