There are, of course, many items that could be placed in a risk register for our ongoing management of COVID-19. I find myself drawn to those categorizable as, or perhaps triggered by, human perception and behavior. By way of limiting the scope of this post to reasonable attention spans, here are my current top 3:
International Affairs
SARS-CoV2/COVID-19 Update, Easter 2020 edition
There are lots of hopeful reports — despite the USA COVID-19 infections being over 1/2 million and the total deaths of over 20,000 people — that the pandemic will soon be “Over.”
This is fantasy thinking at best. SARS-CoV2/COVID-19 won’t be over, until it is over, for YEARS.
“Over” being defined as world wide mass vaccinations to the tune of 70% of humanity or human herd immunity. Assuming such a thing is possible, which it may not be, given this recent report from the UK Daily Mail on post SARS-CoV2/COVID-19 infection immunity —
Blow to Britain’s hopes for coronavirus antibody testing as study finds a THIRD of recovered patients have barely-detectable evidence they have had the virus already
.
– Nearly third of patients have very low levels of antibodies, Chinese study found
– Antibodies not detected at all in 10 people, raising fears they could be reinfected
– Explains why UK Government repeatedly delayed rolling them out to the public.
.
Related studies:
Wu F et al. Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications. medRxiv 2020.03.30.20047365; doi: https://doi.org/10.1101/2020.03.30.20047365.
and
.
Zhao J et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019, Clinical Infectious Diseases, , ciaa344, https://doi.org/10.1093/cid/ciaa344
total by July 1st 51,197
Or this South Korean story on coronavirus “reactivation” —
South Korea reports recovered coronavirus patients testing positive again
APRIL 10, 2020
Josh Smith, Sangmi Cha.
The issue with most COVID-19 tests, like the ones mentioned in South Korea, is they detect SARS-CoV2 RNA. They do not detect whether the viral particles are active or not. The issue here is whether these people are shedding active viral particles that can re-infect people. We don’t know if that is the case here from the story text. Given how infectious it is. This coronavirus will tell us in due course.
There are some viral diseases like Herpes that hide inside your body and reactivate to make you infectious. We do not know enough about the SARs-CoV2 virus to say whether that is the case here.
If the SARS-CoV2 virus is like Herpes in that once contracted, it never goes away and flares infectious several times a year.
And there is no herd immunity for some people no matter how often they are infected.
Then we will need multiple, cheap, out-patient style “cure-treatments” as well as multiple vaccines, based on co-morbidities, and possibly to account for racial differences like sickle cell blood mutations, as SARS-CoV2 may well be more a blood disease than a respiratory infection in terms of it’s killing mechanism.
See:
COVID-19: Attacks the 1-Beta Chain of Hemoglobin and Captures the Porphyrin to Inhibit Human Heme Metabolism
There is not enough reliable data, d*mn it!
Until we get to “Over,” our old economic world of Just-In-Time, Sole Source anywhere, but especially in China, is dead without replacement.
The world is in the same position as Germany was from August 1944 – April 1945 or Japan from August 1944 until August 1945 versus the Allied strategic bombing campaign. We have entered the world of “End Run Production“ as world wide supply chains grind to a halt from various fiddly bits of intermediate parts running out without replacement. The on-and-off hotspots world wide of COVID-19 at different times and places in the world economy is no different than WW2 strategic bombing in terms of causing random damage to the economic life support.
See also “End Run Production” here from this one volume WW2 history book The Great Crusade:
Be it automobiles, self propelled construction equipment, jets, power plants or the latest electronic gadget, anything that has thousands of parts sourced world wide with lots of Chinese cheap/disposable sub-component content anywhere in the supply chain simply won’t be produced for the next 18 months to three years.
This “random damage to the economic life support” effect is amplified by the unwillingness of Western private industry to invest in building the capitol equipment to produced those intermediate parts. Because of the threat of China coming back with predatory pricing — using bought politicians to cover for them — means those parts won’t be built without massive cost plus contract government buy out of the investment risk like happened in the USA in the 1942 WW2 mobilization.
The story of one American n95 mask manufacturer’s experience with the Obama Administration in 2009 with the Swine flu is a case in point. The n95 mask is a 50 cent item where China pays 2 cents a mask for labor versus 10 cents a mask for American labor. When the American manufacturer geared up to replace Chinese mask production. China came back on-line and the Obama Administration refused to keep buying the American mask producer’s 8 cents more expensive mask when the Chinese masks were available.
Unlike almost 80 years ago, current Western and particularly American politicians are too corrupt to go too massive cost plus contract government buy out this private investment risk. Mainly because these political elites can’t be bothered to figure out their 10% cut. Instead we are getting more “fiscal stimulus” AKA boondoggles that the elites will saddle the rest of us with high interest payments on huge public debts.
It will take local small to mid-sized business to get the American economy going during the COVID-19 pandemic via making products and services that don’t use the intermediate products China threatens with when the pandemic ends.
My read on what comes next economically is local/distributed production with limited capitol investment that is multi-product capable. The name for that is additive manufacturing, AKA 3D Printing. Here are a couple of examples:
- The idea of 3D Printed Sand Casting Molds For Automobile Production
voxeljet enters alliance to industrialize core tooling production using 3D printing
2. And the replacement of physical inventory with 3D printers, print media and electronic drawings:
Such “Make or buy” decisions have always been the key decision of any business. The issue here is that middle men wholesalers and in-house warehousing holding cheap Chinese-sourced intermediate parts are both set to go the way of the Doe-Doe Bird in a 3D/AM manufacturing dominated world.
.
Distributed production in multiple localities with 3D/AM vendors for limited runs of existing intermediate products to keep production lines going. Or the re-engineering intermediate products so one 3D/AM print replaces multiple intermediate products for the same reason, will be the stuff of future Masters of Business Administration (MBA) papers describing this imminent change over.
.
But, like developing SARS-CoV2/COVID-19 vaccines, this new locally distributed manufacturing economy will take time. The possible opening of the American economy in May 2020 will not bring the old economy of December 2019 back.
.
That economy is dead. It cannot, will not, come back.
.
We will have to dance with both the sickness from SARS-CoV2/COVID-19 and the widening “End Run Production“ product shortages that the death of the globalist just-in-time, sole source in China economic model causes for years.
.
And this is a hard reality, not a fantasy, we must all face.
In Medias Res
What I’ve got so far:
- Everything’s on the table. The likelihood that your preexisting ideology or priorities are an entirely adequate match to what this situation truly requires of us is close to nil. “In a time of drastic change it is the learners who inherit the future. The learned usually find themselves equipped to live in a world that no longer exists.” ”• Eric Hoffer
- That said, your life experience will give you insights. Privilege your experience over your ideology and nominal priorities.
- All disasters are local. Concentrate on your meaningfully immediate environment, which in this case will be the local market for medical resources. For most of the US, that will be our MSA. For those outside an MSA (metropolitan or micropolitan) that will be their county; and for some it will be the group of counties that feed into the one hospital in the region.
- Deprioritize pandemic news from outside your local area. There are people in the massive NY/NJ/MA outbreak that I worry about, but what happens there will only modestly resemble what happens in the KC MSA, not least because of the difference in population density, which can approach 20x.
- Mitigate or avoid your own risk (including the risk you pose to others) by both following the hygiene advice we’ve all heard and minimizing your physical interaction with anyone outside your immediate household. Internalize Râ‚€ = b × k × d, where Râ‚€ is the reproduction number of the virus, b is the probability of infection given contact with an infectious person, k is the contact rate, and d is the infectious duration. While the nominal Râ‚€ of COVID-19 is ~3, your personal Râ‚€ can be driven to < 1 by your own behavior.
- The general form of the challenge confronting us is abrupt wide variation in formerly relatively constant phenomena. In Talebian terms, we have migrated from “mediocristan” to “extremistan.” The multiplicative nature of a novel viral pandemic, especially by comparison to the relatively predictable seasonality of influenza viruses, has a thick-tailed (power law) probability structure and complex payoffs (notoriously ranging from large numbers of nearly asymptomatic cases to abruptly life-threatening “cytokine storm” reactions). For detail, see The Fourth Quadrant: A Map of the Limits of Statistics.
- So we find ourselves at serious risk of running out of ventilators, ICU beds, and even hospital beds generally, to say nothing of supplies (but see “all disasters are local,” above), raising the prospect of significant second-order mortality among those unable to obtain adequate care for entirely unrelated illnesses and injuries.
- In this connection, many prior customs, techniques, tools, and materials are being revealed as highly dysfunctional and, if all goes sufficiently well, will be swept into the dustbin of history. The bad news for me is that my earlier fears about easily-bottlenecked processes have been realized. But we may look forward to significant adaptation, including deregulation of medical services.
- Similarly, a large number of purported fixes and remedies will fail. Folk remedies, in particular, seem likely to be disastrous, and this blog’s audience needs no persuasion that attempts at central planning will fail thanks to the Hayekian local knowledge problem. In that connection, and to quote something I wrote a few years back: “John Gilmore famously said that ‘the Net interprets censorship as damage and routes around it.’ The future adaptation of representative democracies will depend on our capability, as individuals, to interpret endemic institutional dysfunctionality as damage and route around it.”
- The relatively vulnerable are closer to the center of the network: affluent, living in high-density major cities, well-traveled, extroverted, socially active, with large numbers of regular contacts (even if mostly in a “bubble” as per Murray’s notorious quiz). But some are the alienated and defiant who reject risk avoidance or even risk mitigation tactics (or attempt folk remedies instead), ordinarily associated with …
- The relatively invulnerable, who are at or near the edge of the network: impoverished, living in rural or low-density metro areas, untraveled, introverted, socially isolated, rarely in face-to-face contact with others. Many of these people have mental health issues and associated substance abuse problems. But the relatively invulnerable are also the intelligent and conscientious who promptly adopt appropriate risk management strategies.
- The post-pandemic preferences of the relatively invulnerable will have massive economic and cultural effects. I expect a reasonably quick partial recovery from the economic shutdown, but full recovery may take several years. Many of the “third places” which have done well over the last few decades will not regain their patronage, and as of early April 2020, we can only guess which ones. Fond hopes of some of my co-religionists aside for a sudden revival, I believe church attendance and involvement will be well down in the aftermath, and will not significantly grow until the next “Awakening,” which per Strauss and Howe should occur at mid-century. Until then, believers will be culturally marginalized and congregations will be smaller—but comprised of relatively fervent, active members.
- Geopolitical risks are heightened, especially US-China tensions, and if Xenakis’ “58-year hypothesis” holds, this very year will see an echo of the Cuban Missile Crisis.
- The most important output of this process—and it is a process, with inputs, providers, outputs, recipients, etc—will be a collective lessons-learned database, comprised of both tacit and explicit knowledge, and somehow transmitted to future generations.
Texas Aggie Doctor Reports — Clinical Pearls Covid 19 for ER practitioners
The following information is from a front line ER doctor using the handle of ‘nawlinsag’ on a Texas Aggie web site. I’ve included the link below. I’ve also included the complete text of his post in full in hopes medical professionals and lay people could get the most benefit from his observations of the course of COVID-19 in a small front line Louisiana hospital.
Short form: This is not the flu. It is a horror show of death and disablement that is crowding out all other medical care including an immediate downgrade of life saving cardiac care. Only on in seven people put on ventalators in this hospital is surviving, and then only after 10-t0-12 days of ventalator support.
—–
I just spent an hour typing a long post that erased when I went to change the title so I apologize to the grammar and spelling police. This one will not be proofread and much shorter.
I am an ER MD in New Orleans. Class of 98. Every one of my colleagues have now seen several hundred Covid 19 patients and this is what I think I know.
Clinical course is predictable.
2-11 days after exposure (day 5 on average) flu like symptoms start. Common are fever, headache, dry cough, myalgias(back pain), nausea without vomiting, abdominal discomfort with some diarrhea, loss of smell, anorexia, fatigue.
Day 5 of symptoms- increased SOB, and bilateral viral pneumonia from direct viral damage to lung parenchyma.
Day 10- Cytokine storm leading to acute ARDS and multiorgan failure. You can literally watch it happen in a matter of hours.
81% mild symptoms, 14% severe symptoms requiring hospitalization, 5% critical.
Patient presentation is varied. Patients are coming in hypoxic (even 75%) without dyspnea. I have seen Covid patients present with encephalopathy, renal failure from dehydration, DKA. I have seen the bilateral interstitial pneumonia on the xray of the asymptomatic shoulder dislocation or on the CT’s of the (respiratory) asymptomatic polytrauma patient. Essentially if they are in my ER, they have it. Seen three positive flu swabs in 2 weeks and all three had Covid 19 as well. Somehow this ***** has told all other disease processes to get out of town.
China reported 15% cardiac involvement. I have seen covid 19 patients present with myocarditis, pericarditis, new onset CHF and new onset atrial fibrillation. I still order a troponin, but no cardiologist will treat no matter what the number in a suspected Covid 19 patient. Even our non covid 19 STEMIs at all of our facilities are getting TPA in the ED and rescue PCI at 60 minutes only if TPA fails.
Diagnostic
CXR- bilateral interstitial pneumonia (anecdotally starts most often in the RLL so bilateral on CXR is not required). The hypoxia does not correlate with the CXR findings. Their lungs do not sound bad. Keep your stethoscope in your pocket and evaluate with your eyes and pulse ox.
Labs- WBC low, Lymphocytes low, platelets lower then their normal, Procalcitonin normal in 95%
CRP and Ferritin elevated most often. CPK, D-Dimer, LDH, Alk Phos/AST/ALT commonly elevated.
Notice D-Dimer- I would be very careful about CT PE these patients for their hypoxia. The patients receiving IV contrast are going into renal failure and on the vent sooner.
Basically, if you have a bilateral pneumonia with normal to low WBC, lymphopenia, normal procalcitonin, elevated CRP and ferritin- you have covid-19 and do not need a nasal swab to tell you that.
A ratio of absolute neutrophil count to absolute lymphocyte count greater than 3.5 may be the highest predictor of poor outcome. the UK is automatically intubating these patients for expected outcomes regardless of their clinical presentation.
An elevated Interleukin-6 (IL6) is an indicator of their cytokine storm. If this is elevated watch these patients closely with both eyes.
Other factors that appear to be predictive of poor outcomes are thrombocytopenia and LFTs 5x upper limit of normal.
COVID-19 Update 2-17-2020
As of this morning’s time hack, world wide there are now 1,770 dead and 71,223 infected by COVID-19. Community spread is underway in Singapore (see chart), Taiwan and Japan. The USA thinks it might be on-going in the USA. Both Japan and the USA refuse to state this, but actions being taken argue otherwise. Two horrid COVID-19 infection reports from Chinese news sources — the Taiwan News is reporting re-infection with COVID-19 is causing heart failure and South China Morning Post is reporting 34 and 94 day from exposure to infection super spreaders. Recovered from COVID-19 infection Ontario couple are still testing positive for coronavirus. Finally, COVID-19 fomit** contamination of Chinese money and survival of corona-virus in high heat & humidity are also in the update.
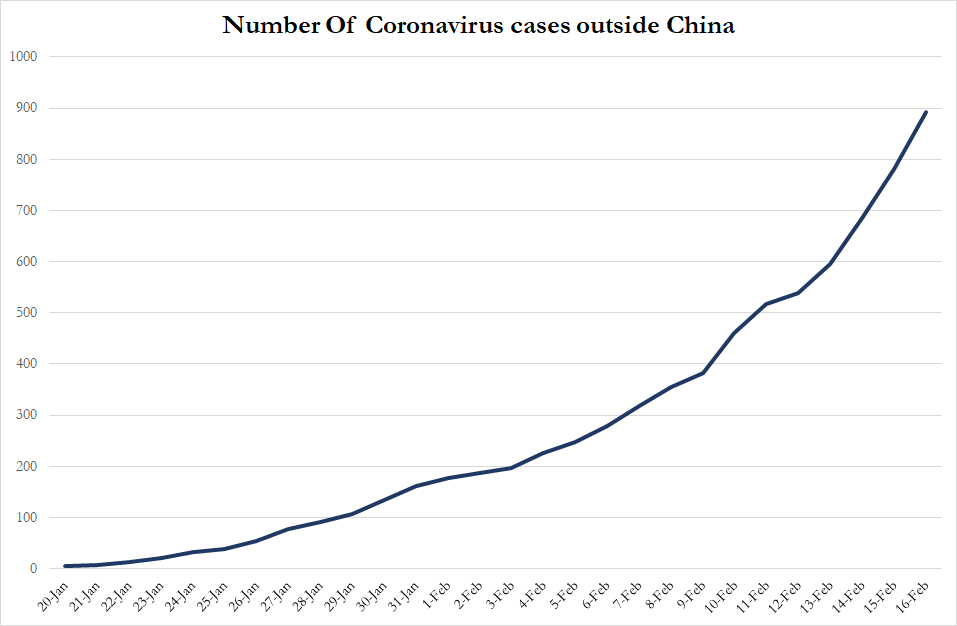
Number of COVID-19 Infections outside China as of Feb 16, 2020
