As I retired from a relatively uneventful career in the peacetime Air Force in 1997, I’ve been out of the military for longer than I was in it. I don’t hang around so much in military veteran circles online as I did early in the decade afterwards, when my daughter was serving in the Marines after 9/11 and deployed to Kuwait and Iraq. But she does venture into veteran social media circles, on a local basis through organizations and outlets like Bourbiz, Grunt Style, Ranger Up, and Black Rifle Coffee … and she called my attention to what amounts to a dumpster fire ongoing in veteran circles. Holy heck, it’s more a raging nuclear inferno than your plain ordinary social media dumpster fire. Read the series of articles, she said, it’s jaw-dropping and so I did. Oh. My. G*d. I thought the Vietnam-era “stolen valor” incidents so thoroughly documented in this book were the far frozen limit, but this Steele character appears to have ventured into hitherto unexplored dimensions.
Military Affairs
This Post Has Absolutely Nothing to do with Coronavirus
The US Naval Institute has posted some links to their archives. This one is interesting: a 1912 think piece on the future of the submarine, written by then-lieutenant C W Nimitz.
In Medias Res
What I’ve got so far:
- Everything’s on the table. The likelihood that your preexisting ideology or priorities are an entirely adequate match to what this situation truly requires of us is close to nil. “In a time of drastic change it is the learners who inherit the future. The learned usually find themselves equipped to live in a world that no longer exists.” ”• Eric Hoffer
- That said, your life experience will give you insights. Privilege your experience over your ideology and nominal priorities.
- All disasters are local. Concentrate on your meaningfully immediate environment, which in this case will be the local market for medical resources. For most of the US, that will be our MSA. For those outside an MSA (metropolitan or micropolitan) that will be their county; and for some it will be the group of counties that feed into the one hospital in the region.
- Deprioritize pandemic news from outside your local area. There are people in the massive NY/NJ/MA outbreak that I worry about, but what happens there will only modestly resemble what happens in the KC MSA, not least because of the difference in population density, which can approach 20x.
- Mitigate or avoid your own risk (including the risk you pose to others) by both following the hygiene advice we’ve all heard and minimizing your physical interaction with anyone outside your immediate household. Internalize Râ‚€ = b × k × d, where Râ‚€ is the reproduction number of the virus, b is the probability of infection given contact with an infectious person, k is the contact rate, and d is the infectious duration. While the nominal Râ‚€ of COVID-19 is ~3, your personal Râ‚€ can be driven to < 1 by your own behavior.
- The general form of the challenge confronting us is abrupt wide variation in formerly relatively constant phenomena. In Talebian terms, we have migrated from “mediocristan” to “extremistan.” The multiplicative nature of a novel viral pandemic, especially by comparison to the relatively predictable seasonality of influenza viruses, has a thick-tailed (power law) probability structure and complex payoffs (notoriously ranging from large numbers of nearly asymptomatic cases to abruptly life-threatening “cytokine storm” reactions). For detail, see The Fourth Quadrant: A Map of the Limits of Statistics.
- So we find ourselves at serious risk of running out of ventilators, ICU beds, and even hospital beds generally, to say nothing of supplies (but see “all disasters are local,” above), raising the prospect of significant second-order mortality among those unable to obtain adequate care for entirely unrelated illnesses and injuries.
- In this connection, many prior customs, techniques, tools, and materials are being revealed as highly dysfunctional and, if all goes sufficiently well, will be swept into the dustbin of history. The bad news for me is that my earlier fears about easily-bottlenecked processes have been realized. But we may look forward to significant adaptation, including deregulation of medical services.
- Similarly, a large number of purported fixes and remedies will fail. Folk remedies, in particular, seem likely to be disastrous, and this blog’s audience needs no persuasion that attempts at central planning will fail thanks to the Hayekian local knowledge problem. In that connection, and to quote something I wrote a few years back: “John Gilmore famously said that ‘the Net interprets censorship as damage and routes around it.’ The future adaptation of representative democracies will depend on our capability, as individuals, to interpret endemic institutional dysfunctionality as damage and route around it.”
- The relatively vulnerable are closer to the center of the network: affluent, living in high-density major cities, well-traveled, extroverted, socially active, with large numbers of regular contacts (even if mostly in a “bubble” as per Murray’s notorious quiz). But some are the alienated and defiant who reject risk avoidance or even risk mitigation tactics (or attempt folk remedies instead), ordinarily associated with …
- The relatively invulnerable, who are at or near the edge of the network: impoverished, living in rural or low-density metro areas, untraveled, introverted, socially isolated, rarely in face-to-face contact with others. Many of these people have mental health issues and associated substance abuse problems. But the relatively invulnerable are also the intelligent and conscientious who promptly adopt appropriate risk management strategies.
- The post-pandemic preferences of the relatively invulnerable will have massive economic and cultural effects. I expect a reasonably quick partial recovery from the economic shutdown, but full recovery may take several years. Many of the “third places” which have done well over the last few decades will not regain their patronage, and as of early April 2020, we can only guess which ones. Fond hopes of some of my co-religionists aside for a sudden revival, I believe church attendance and involvement will be well down in the aftermath, and will not significantly grow until the next “Awakening,” which per Strauss and Howe should occur at mid-century. Until then, believers will be culturally marginalized and congregations will be smaller—but comprised of relatively fervent, active members.
- Geopolitical risks are heightened, especially US-China tensions, and if Xenakis’ “58-year hypothesis” holds, this very year will see an echo of the Cuban Missile Crisis.
- The most important output of this process—and it is a process, with inputs, providers, outputs, recipients, etc—will be a collective lessons-learned database, comprised of both tacit and explicit knowledge, and somehow transmitted to future generations.
The Beginning of the Okinawa Campaign — Plus 75 years
In the press of events related to the Great Wuhan Coronavirus Pandemic, many anniversaries of the Second World War have been passing by with little notice and less comment. For example, April 1st 2020 was the 75th Anniversary of the April 1st 1945 “Love-Day” landings on the western shores of Okinawa.
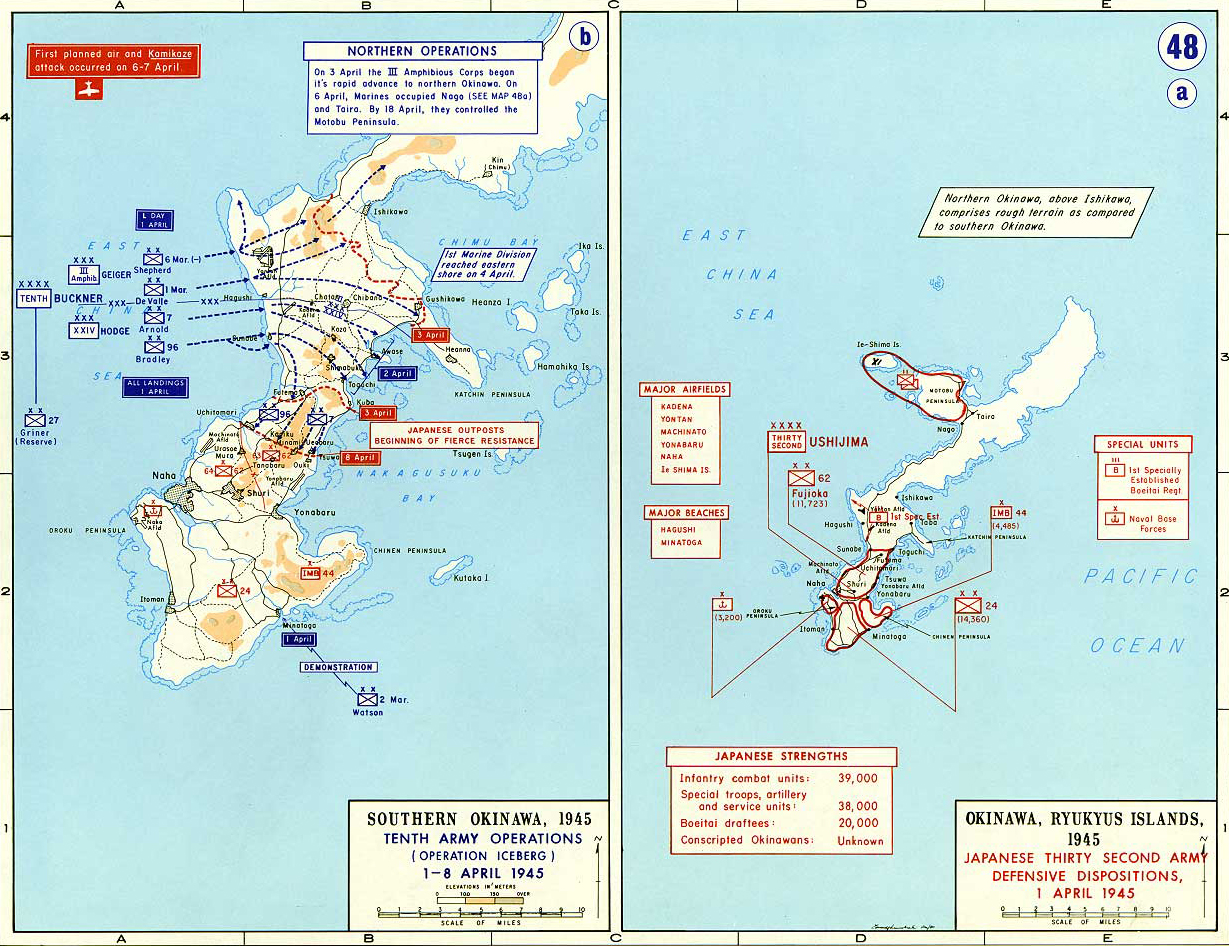
The Okinawa campaign in WW2 has often been described as marking the end old style total war. Where “cork screw and blow torch” close combat to the death between American attackers “who fought to live” and Japanese defenders who “died in order to fight” played out its last dance.

Upon closer examination, as this 75th anniversary article series will demonstrate, Okinawa is far better described as a high tech war for the electromagnetic spectrum between technological peer competitors air and naval forces. A “secret radar war,” if you will, where two opposing command, control, communications and intelligence (C3I) sensor networks were directing land, sea and air forces in a series of both combat and logistical moves and countermoves.
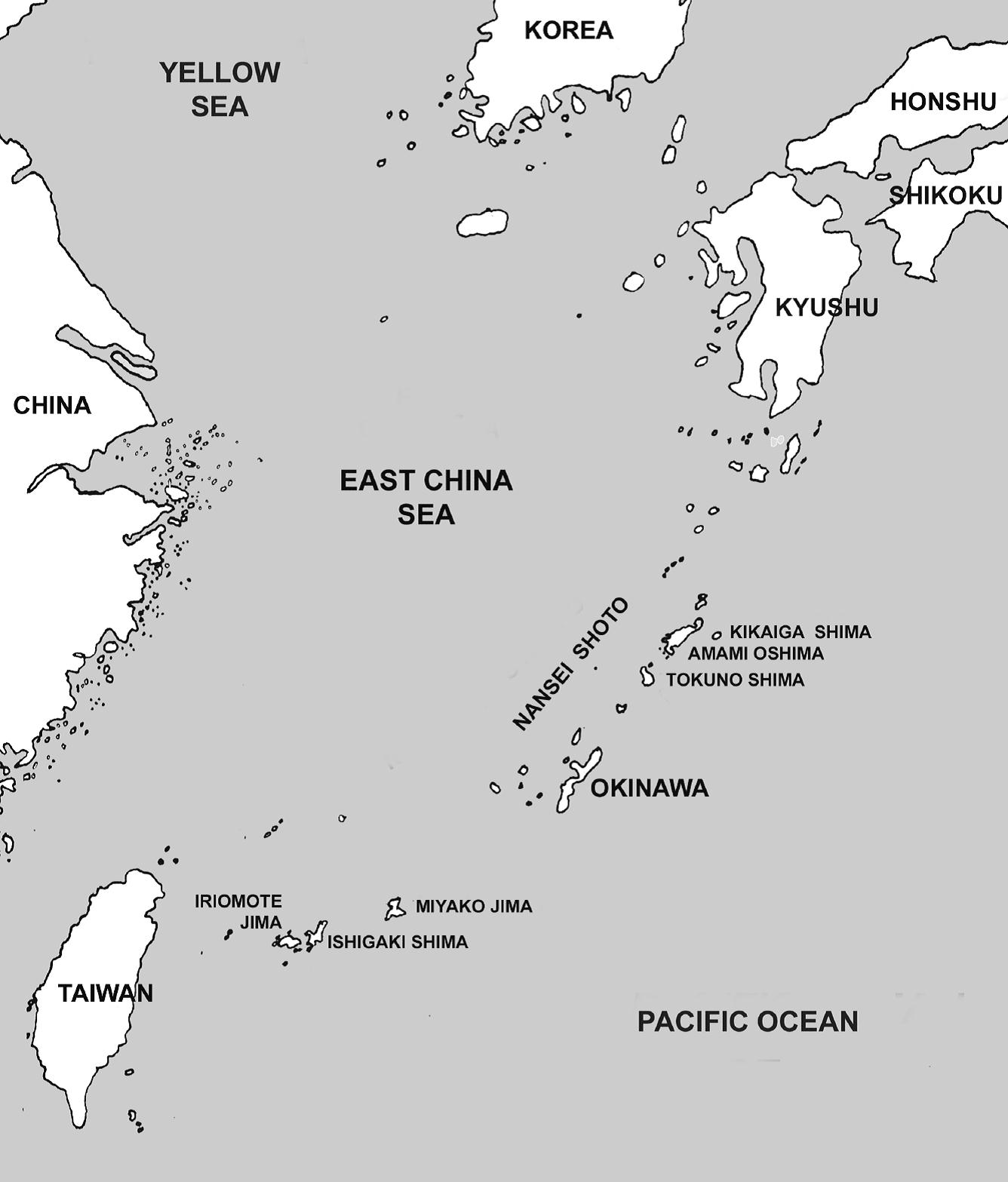
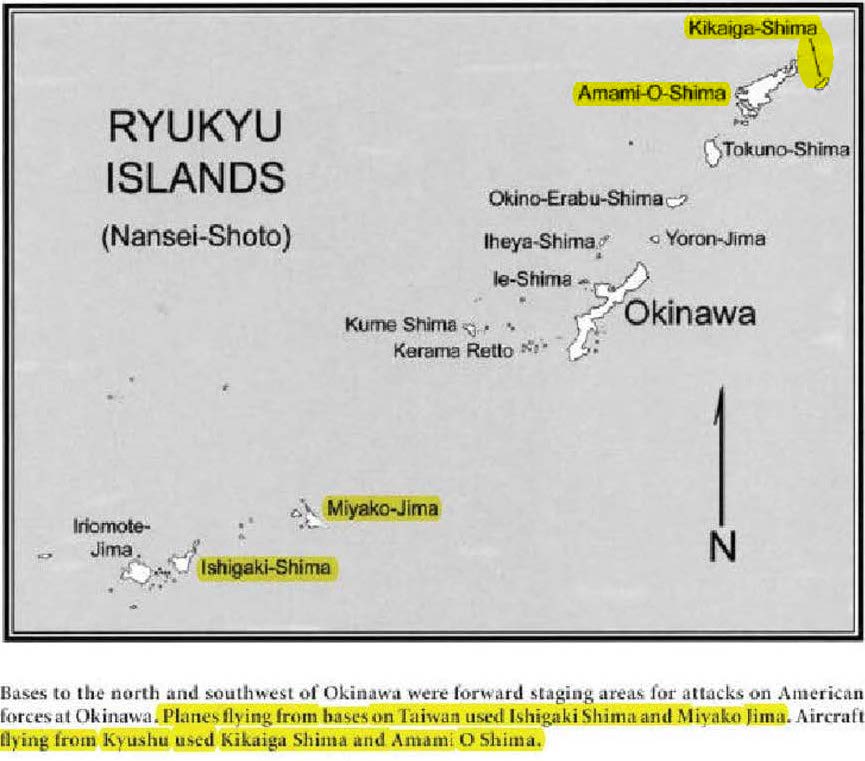
And while the less advanced, and organizationally deficient, Japanese military lost Okinawa proper. It still took advantage of the primarily US Navy institutional biases, American military inter-service rivalries, logistical planning weaknesses caused by that rivalry and US Navy’s unwillingness to learn from “non-approved” sources to never the less defeat the US Navy’s original Phase III plan to overrun the upper Ryukyu’s and install island air and radar bases close enough Kyushu to properly provide land based air superiority for the invasion of Japan.
These campaign objective failures were hidden in tales of US Navy destroyer picket heroism in the “Fleet That Came to Stay:…and classified top secret files…because of the coming budget war associated with the pending merger of the War and Navy department’s into the Department of Defense. After 75 years, this series will part the curtains on these hidden histories.
Too accomplish that objective, this series will examine the planned goals of the Operation Iceberg campaign against what was accomplished. How various American military institutions, doctrine and planning failed. And why the defeat of the US Navy’s Phase III plans set the stage for an American blood bath of preventable naval casualties during the planned Operation Olympic assault of the Japanese home islands, had the atomic bombings of Hiroshima and Nagasaki not made the invasion of Japan unnecessary.
Texas Aggie Doctor Reports — Clinical Pearls Covid 19 for ER practitioners
The following information is from a front line ER doctor using the handle of ‘nawlinsag’ on a Texas Aggie web site. I’ve included the link below. I’ve also included the complete text of his post in full in hopes medical professionals and lay people could get the most benefit from his observations of the course of COVID-19 in a small front line Louisiana hospital.
Short form: This is not the flu. It is a horror show of death and disablement that is crowding out all other medical care including an immediate downgrade of life saving cardiac care. Only on in seven people put on ventalators in this hospital is surviving, and then only after 10-t0-12 days of ventalator support.
—–
I just spent an hour typing a long post that erased when I went to change the title so I apologize to the grammar and spelling police. This one will not be proofread and much shorter.
I am an ER MD in New Orleans. Class of 98. Every one of my colleagues have now seen several hundred Covid 19 patients and this is what I think I know.
Clinical course is predictable.
2-11 days after exposure (day 5 on average) flu like symptoms start. Common are fever, headache, dry cough, myalgias(back pain), nausea without vomiting, abdominal discomfort with some diarrhea, loss of smell, anorexia, fatigue.
Day 5 of symptoms- increased SOB, and bilateral viral pneumonia from direct viral damage to lung parenchyma.
Day 10- Cytokine storm leading to acute ARDS and multiorgan failure. You can literally watch it happen in a matter of hours.
81% mild symptoms, 14% severe symptoms requiring hospitalization, 5% critical.
Patient presentation is varied. Patients are coming in hypoxic (even 75%) without dyspnea. I have seen Covid patients present with encephalopathy, renal failure from dehydration, DKA. I have seen the bilateral interstitial pneumonia on the xray of the asymptomatic shoulder dislocation or on the CT’s of the (respiratory) asymptomatic polytrauma patient. Essentially if they are in my ER, they have it. Seen three positive flu swabs in 2 weeks and all three had Covid 19 as well. Somehow this ***** has told all other disease processes to get out of town.
China reported 15% cardiac involvement. I have seen covid 19 patients present with myocarditis, pericarditis, new onset CHF and new onset atrial fibrillation. I still order a troponin, but no cardiologist will treat no matter what the number in a suspected Covid 19 patient. Even our non covid 19 STEMIs at all of our facilities are getting TPA in the ED and rescue PCI at 60 minutes only if TPA fails.
Diagnostic
CXR- bilateral interstitial pneumonia (anecdotally starts most often in the RLL so bilateral on CXR is not required). The hypoxia does not correlate with the CXR findings. Their lungs do not sound bad. Keep your stethoscope in your pocket and evaluate with your eyes and pulse ox.
Labs- WBC low, Lymphocytes low, platelets lower then their normal, Procalcitonin normal in 95%
CRP and Ferritin elevated most often. CPK, D-Dimer, LDH, Alk Phos/AST/ALT commonly elevated.
Notice D-Dimer- I would be very careful about CT PE these patients for their hypoxia. The patients receiving IV contrast are going into renal failure and on the vent sooner.
Basically, if you have a bilateral pneumonia with normal to low WBC, lymphopenia, normal procalcitonin, elevated CRP and ferritin- you have covid-19 and do not need a nasal swab to tell you that.
A ratio of absolute neutrophil count to absolute lymphocyte count greater than 3.5 may be the highest predictor of poor outcome. the UK is automatically intubating these patients for expected outcomes regardless of their clinical presentation.
An elevated Interleukin-6 (IL6) is an indicator of their cytokine storm. If this is elevated watch these patients closely with both eyes.
Other factors that appear to be predictive of poor outcomes are thrombocytopenia and LFTs 5x upper limit of normal.